This Week in Dental Implants we wanted to focus on dental implant robotic surgery. With continued rapid advancements in AI (see AI in Implant Dentistry: Some Interesting Studies, and other underlying technologies, it seems inevitable that robotic surgery, despite the still considerable limitations, will improve and will have a major impact on implant surgery in the years ahead. Even if, for various reasons, the pace of actual clinical adoption is currently slow, we think learning from the attempts at implementation of robotic surgery and the studies on these advanced systems, can vastly improve the current standard surgical techniques.
Background
Robots have shown significant potential in improving the accuracy and efficiency of implant surgery. Currently, there are several robotic systems on the market with one, Yomi, receiving FDA approval in 2017. The difference in the robotic systems are broadly based on the level of interaction required by a surgeon. Briefly, there 3 types of robotic systems: Active (the robot basically does everything), Passive (the robot is guided by a human operation/surgeon), and Semi-Active (kind of combination of the active and passive, where the robot places the implant but the operator guides the robot into the mouth).
Various studies highlight the limitations of and the advantages of robotic systems in dental implant placement, particularly in overcoming the pitfalls of traditional static and dynamic navigation techniques.
According to the most recent meta-analysis study, 1:
Autonomous dental implant robotic surgery has shown to be feasible for placing implants in both partially and completely edentulous patients, achieving consistent mean linear and angular deviations of approximately 0.6 mm and 1.40°, respectively. However, clinical practicality of autonomous dental implant robotic surgery remained cumbersome, with well-trained operators needed to plan and assist ADIR procedures and a technical expert providing backup control
Earlier clinical studies share similar positivity regarding results, with some hesitation on the need for further studies.
Autonomous robots exhibit exceptional accuracy by accurately controlling axial and angular errors. It can improve the accuracy of implant surgery, which may become a key technology for changing implant surgery. However, further clinical trials are still needed to provide a basis for the rapid development of robotic surgery field. 2
For exceptional reviews of the entire state of robotic implant surgery, please see Robot-assisted dental implant surgery procedure: A literature review 10 and Accuracy and operation procedure of robotic computer-aided implant surgery 11
In summary, the evidence suggests that robots can indeed improve implant surgery by providing greater precision, reducing human error, and facilitating more efficient surgical procedures. However, the current limitations include, but are not limited to: cost (a huge factor), difficulty in accessing hard-to-reach areas, and an ability to manage complex cases, particularly those with poor bone. These systems also require extensive training of surgeons and assistants so they can properly use the technology to reduce the risk of errors. It seems like these limitations might be reduced in the years ahead, as AI advances and is incorporated into existing and new robotic systems.
Case Photos
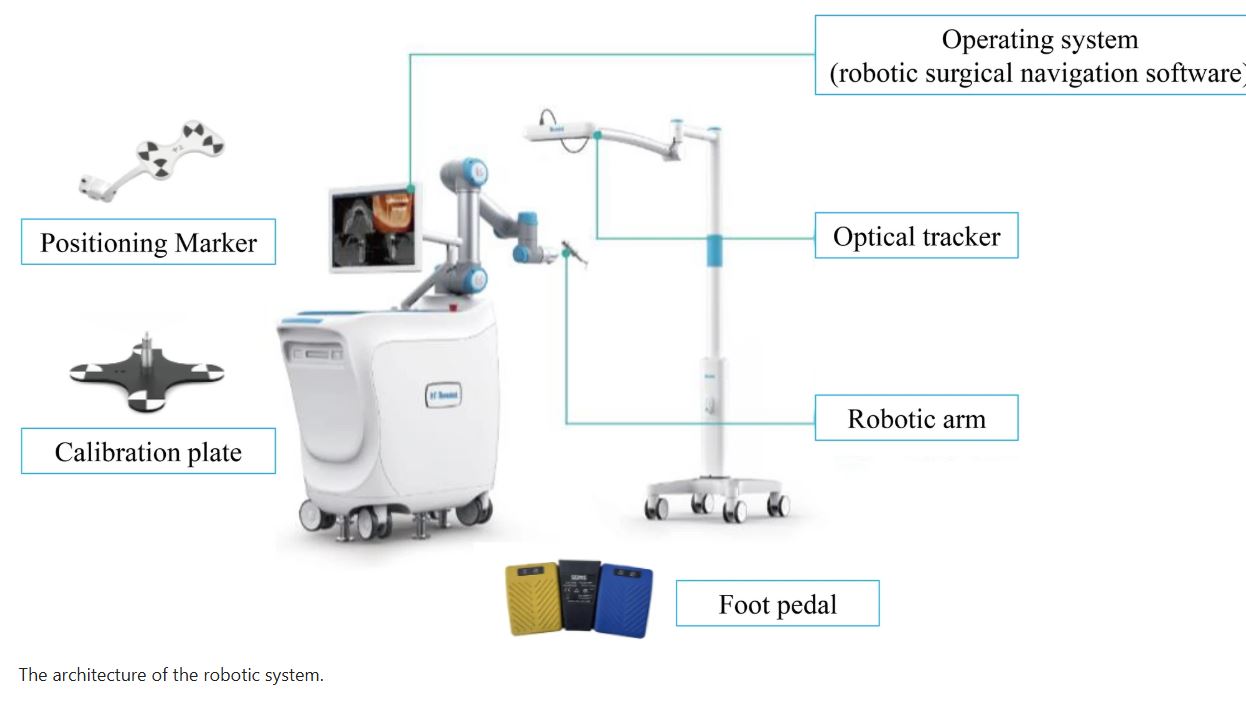
The Remebot robotic system (Remebot, Baihui Weikang Technology Co., Ltd, Beijing, China) is comprised of three main parts: a robot arm with a terminal executor, an optical tracker, and an operating system
Case below by: Liu, Y., Zheng, Q., Xu, Z. et al. Accuracy and operation procedure of robotic computer-aided implant surgery

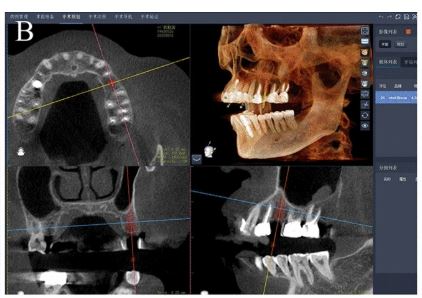

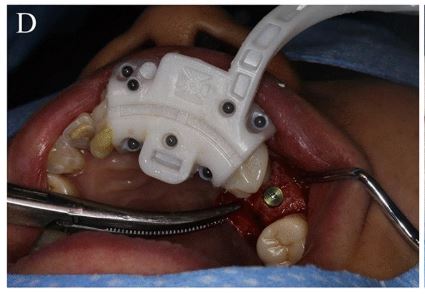

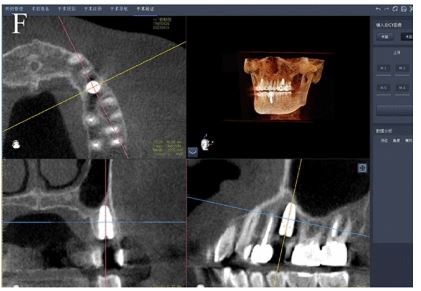
Surgical process of robotic system and postoperative assessment. (A ), The positioning marker was fixed to the residual teeth. (B ), Preoperative planning in the robotic navigation software. (C ), The implant osteotomy was automatically performed by the robotic system. (D ), Dental implant insertion. (E ), The positioning marker was removed. (F ), Postoperative assessment of the deviations between the planned and achieved implants
Case by: Liu, Y., Zheng, Q., Xu, Z. et al. Accuracy and operation procedure of robotic computer-aided implant surgery
Case 2
Case below by: Yang S, Chen J, Li A, Li P, Xu S. Autonomous Robotic Surgery for Immediately Loaded Implant-Supported Maxillary Full-Arch Prosthesis: A Case Report
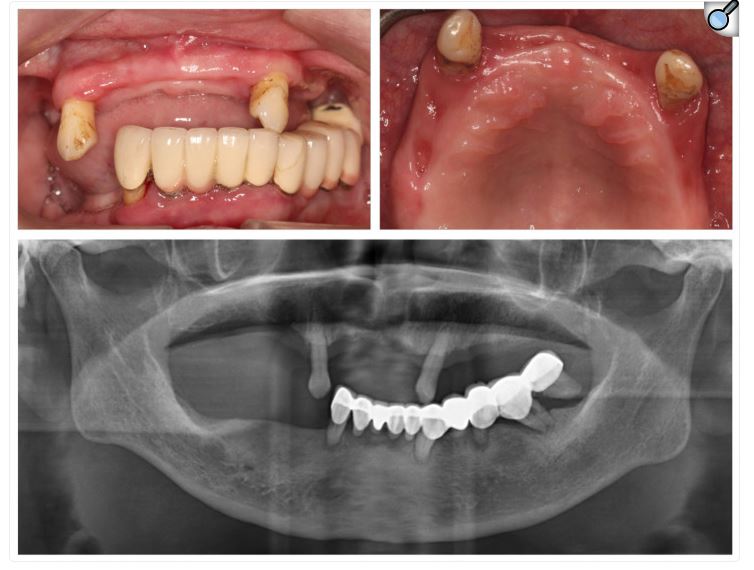
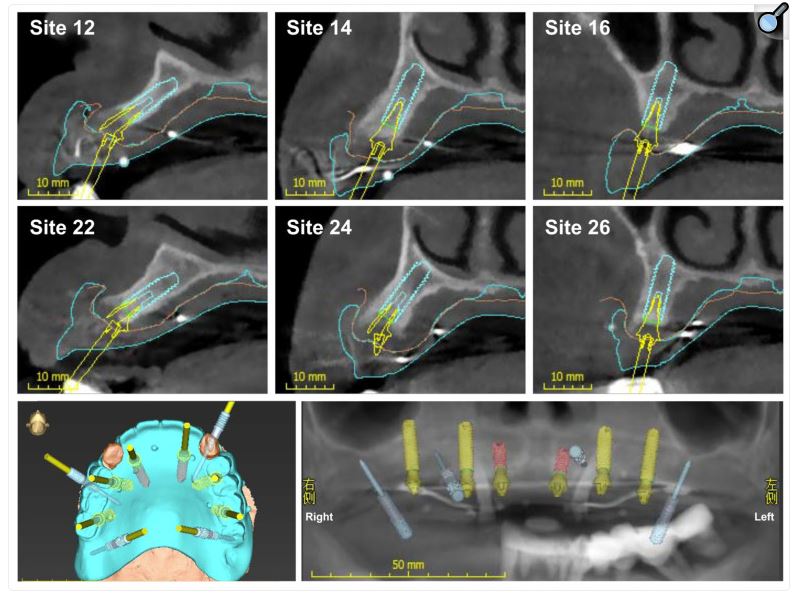
Virtual 3D planning positions for placing six implants and four metallic pins in the maxilla. In the panoramic radiograph, red implants show a diameter of 3.4 mm, yellow implants indicate a diameter of 4.0 mm, and blue ones represent metallic pins.
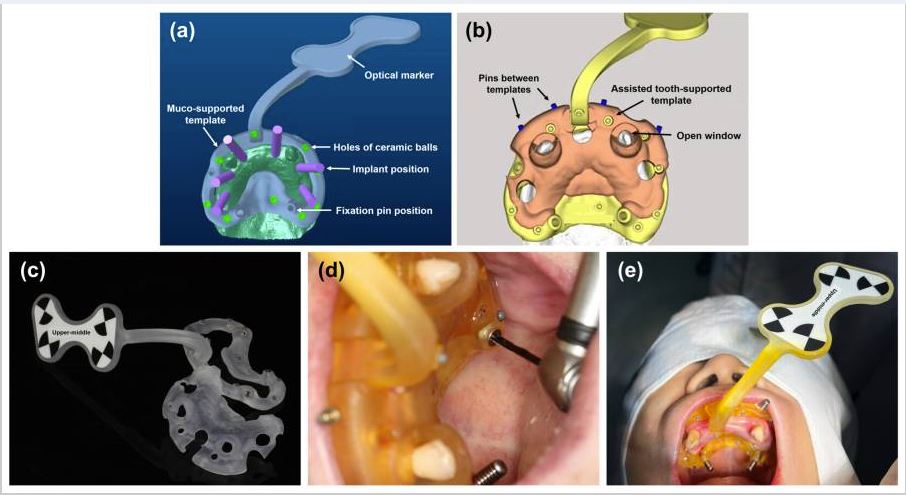
Design, fabrication, and fixation of the customized surgical template with positioning marker. (a ) Design of the marker template; (b ) design of the tooth-supported guide template; (c ) 3D-printed surgical templates; (d ) the fixation of templates; and (e ) the patient with the surgical marker template.
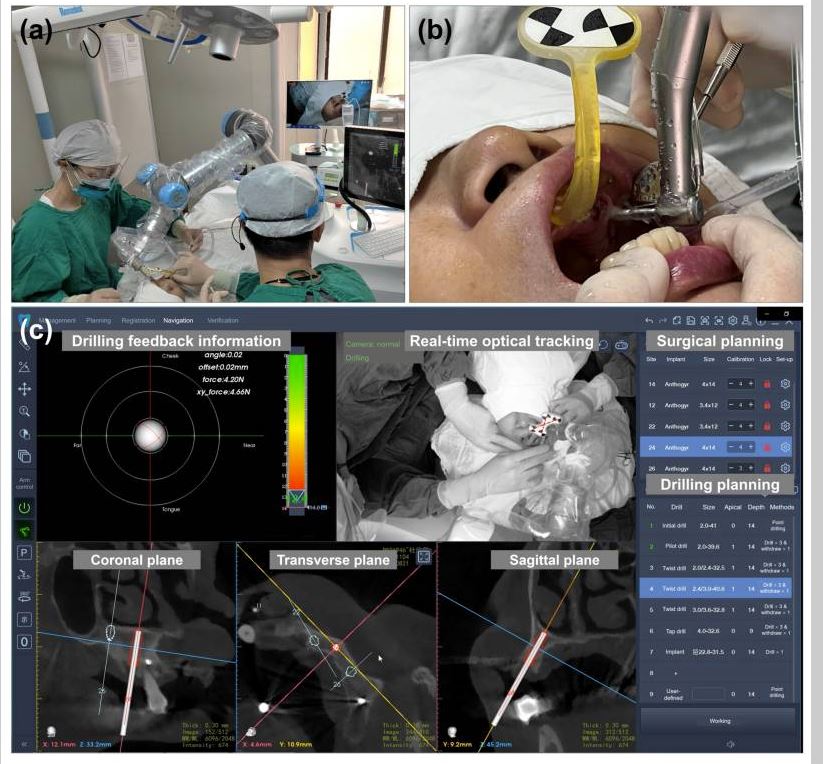
Intraoperative image and autonomous osteotomy procedure. (a ) The autonomous implant osteotomy was performed by the image-guided robotic surgery system; (b ) autonomous implant osteotomy at site #24; and (c ) robot-assisted surgical software system.
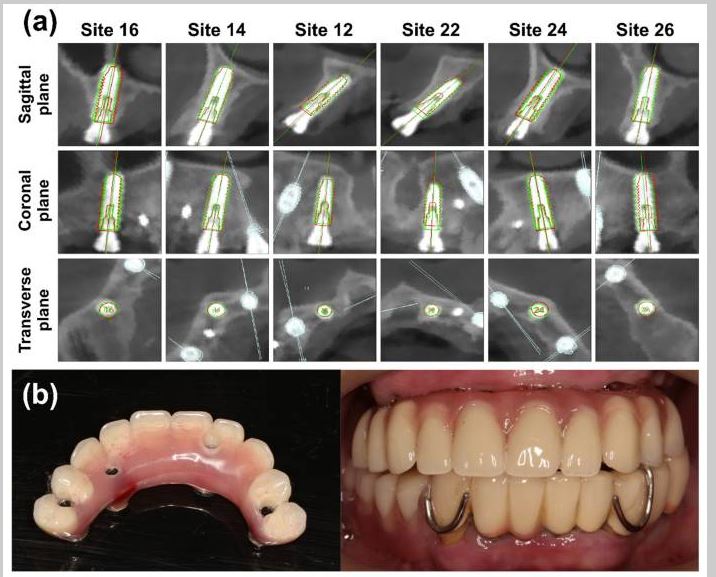
Postoperative evaluation. (a ) Accuracy analysis for deviations between the planned and placed implants. The red profile indicates the planned implant, and the green profile shows the placed implant; (b ) the immediately loaded provisional reconstruction.
References
1. In-Vivo Accuracy of Autonomous Dental Implant Robotic Surgery: Systematic Review and Meta-Analysis., Alessandro Pozzi , Paolo Carosi , Claudia Lorenzi , James Chow , Hom-Lay Wang , German O Gallucci , The International journal of oral & maxillofacial implants. Volume: 0, Issue: 0, 2025
OBJECTIVES
To systematically analyze the accuracy of autonomous dental implant robotic (ADIR) surgery for dental implant placement.
MATERIALS AND METHODS
PubMed, Embase, and Cochrane CENTRAL were searched on February 21, 2024. Any clinical studies with exception of case reports, assessing ADIR accuracy by superimposing pre-op digital planning with post-op CBCT, were included. The risk of bias was assessed, and a meta-analysis was performed using a random-effect model to evaluate linear and angular deviations between planned and placed implants.
RESULTS
Data from 6 clinical studies reporting ADIR accuracy in 96 patients with 299 dental implants included (102 in 69 partial edentates, 197 in 27 complete-arch scenarios). The meta-analysis at implant level reported a mean overall accuracy of ADIR of 0.60 mm 95% CI [0.5133; 0.6965] at platform, 0.63 mm 95% CI [0.5663; 0.6909] at apex, and 1.242° 95% CI [1.2182; 1.6320] of angular deviation. ADIR accuracy resulted significantly higher than s- and d-CAIS.
CONCLUSION
Within the limitations of this review, autonomous dental implant robotic surgery has shown to be feasible for placing implants in both partially and completely edentulous patients, achieving consistent mean linear and angular deviations of approximately 0.6 mm and 1.40°, respectively. However, clinical practicality of autonomous dental implant robotic surgery remained cumbersome, with well-trained operators needed to plan and assist ADIR procedures and a technical expert providing backup control. Read More
2. Exploring the Learning Curve of Dental Implant Placement Using a Task-Autonomous Robotic System Among Young Dentists From Different Specialties-A Pilot Module Study., Minjie Zhuang , Jinyan Chen , Baoxin Tao , Meisha Gul , Feng Wang , Yiqun Wu , Clinical implant dentistry and related research. Volume: 27, Issue: 1, 2025
BACKGROUND
The learning curve effect of dynamic computer-assisted implant surgery (D-CAIS) was observed among inexperienced novice surgeons. The learning curves can provide valuable information for novice surgeons and valid comparisons between new and conventional techniques. Recently, robotic computer-assisted implant surgery (R-CAIS) has shown promise as a novel dental implant surgical technique for both partially and edentulous patients. However, its learning curve remains unknown.
PURPOSE
The aim of this study was to explore the learning curve of dental implant placement surgery with a task-autonomous robotic system among young dentists with different specialties.
METHODS AND MATERIALS
Four young dentists (mean age: 25.3 ± 1.5 years at the beginning of their first attempt) with equal representation of males and females and with different specialties participated in this study. None of the participants had prior experience in R-CAIS. Each operator placed eight implants over eight attempts using a semi-active task-autonomous robotic system. Among the eight implants, four were straight lateral incisor implants, and four were 30°-tilted premolar implants. The implants were placed in each dental quadrant of the maxillary and mandibular jaw modules. The operation time was recorded. Coronal, apical, and angular deviations between the planned and actual sites of implant placement were measured by merging preoperative and postoperative cone-beam computed tomography (CBCT) scans. The data were analyzed with repeated-measures ANOVA (α = 0.05).
RESULTS
The mean time for implant placement was associated with the number of attempts (p < 0.01). The time taken for the second attempt was significantly shorter than that of the first attempt (33.26 vs. 30.47 min; p < 0.001) then it plateaued. Three-dimensional (3D) angular (p = 0.31), coronal deviation (p = 0.26), and apical deviation (p = 0.06) did not differ significantly among attempts. The mean values and standard deviations of 3D coronal deviation, 3D apical deviation, and 3D angular deviation were 0.71 ± 0.31 mm, 0.72 ± 0.30 mm, and 0.94 ± 0.58°, respectively. Neither the position of the jaw (p > 0.59) nor the tilt angle of the implant (straight or 30°-tilted, p > 0.85) was related to implant placement accuracy.
CONCLUSIONS
Dentists quickly learned the basic workflow of R-CAIS and thus facilitated the clinicians in the mastery of implant placement on edentulous jaw modules, leading to a comparable operating speed and high precision. Moreover, the accuracy of placement of straight and tilted implants in both the maxilla and mandible with R-CAIS was satisfactory. Read More
3. Case report and literature review: autonomous robotic system assisted palatal implantation at an anterior teeth site compromised by periapical cyst., Xiuyu Liu , Huixin Lv , Meiqing Chen , Siyu Chen , Kewen Jia , Sezhen Quni , Lu Zhang , Yanmin Zhou , Frontiers in medicine. Volume: 11, Issue: , 2024
BACKGROUND
Immediate implant placement (IIP), which preserves gingival height and papilla shape while simultaneously accelerating the implant treatment period, has become a popular method due to its commendable clinical outcomes. Nonetheless, deploying immediate implants demands specific preconditions concerning the remaining alveolar bone. This poses a challenge to the accuracy of implant surgery.
CASE PRESENTATION
In this report, we present the case of a 60-year-old woman with a left upper anterior tooth crown dislodged for over a month. Cone beam computed tomography (CBCT) revealed the absence of a labial bone wall on tooth 22, a remaining 1 mm bone wall on the labial side of the root apex, and a 17.2 mm*8.9 mm*4.7 mm shadow in the periapical region of the root apices of teeth 21 and 22, with the narrowest width on the sagittal plane being approximately 5 mm. After the surgeon removed the cyst, they completed the subsequent implantation surgery using an autonomous robot in a challenging aesthetic area. This method circumvented the potential exposure of the screw thread on the labial implant surface, assured initial implant stability.
CONCLUSION
Five months after the operation, the dental crown was restored. The implant remained stable, with yielding notable clinical results. To the best of our knowledge, this clinical case is the first to report the feasibility and precision of immediate implantation in anterior teeth site with periapical cyst removal, performed by an autonomous robotic surgical system. Autonomous robots exhibit exceptional accuracy by accurately controlling axial and angular errors. It can improve the accuracy of implant surgery, which may become a key technology for changing implant surgery. However, further clinical trials are still needed to provide a basis for the rapid development of robotic surgery field. Read More
4. Accuracy of an autonomous dental implant robotic system versus static guide-assisted implant surgery: A retrospective clinical study., Shasha Jia , Guowei Wang , Yimin Zhao , Xiaojing Wang , The Journal of prosthetic dentistry. Volume: 133, Issue: 3, 2025
STATEMENT OF PROBLEM
The accuracy of implant placement is a prerequisite for prosthetically driven implant surgery and is necessary to ensure the long-term stability of dental implants. Imprecise implant position may bring difficulties for restoration, damage anatomic structures, affect peri-implant tissues, and lead to ultimate implant failure.
PURPOSE
The purpose of this retrospective clinical study was to compare the accuracy of implants placed with an autonomous dental implant robotic (ADIR) system with those placed with static computer assisted implant surgery (sCAIS).
MATERIAL AND METHODS
Thirty-nine participants were enrolled in this retrospective study: 20 participants had received implant surgery with the ADIR system and 19 participants had implants placed with sCAIS. The preoperative plans and postoperative cone beam computed tomography (CBCT) scans after implant placement were matched during the study. The coronal, apical, and angular deviations were measured and analyzed. A linear regression model was established to analyze the source of deviation. MANOVA was used to compare differences in the major outcome variables (α=.05).
RESULTS
A total of 60 implants were placed in 39 participants (30 in each of the 2 groups). The mean ±standard deviation coronal, apical, and angular deviation of the ADIR system group and sCAIS group were 0.43 ±0.18 mm versus 1.31 ±0.62 mm (P<.001), 0.56 ±0.18 mm versus 1.47 ±0.65 mm (P<.001), and 1.48 ±0.59 degrees versus 2.42 ±1.55 degrees (P=.003), respectively. In addition, there was no significant difference in accuracy in the different implant regions (anterior, premolar, molar, maxilla, mandible) (P>.05). No complications were observed.
CONCLUSIONS
The accuracy of the implant position using the ADIR system was significantly higher than with sCAIS, suggesting that the ADIR system can achieve minimally invasive and excellent accuracy. In addition, implant regions had no significant influence on the accuracy of implant placement. (Keywords: Robotic system, Implant surgery, Static guide, Autonomous, Accuracy). Read More
5. Accuracy of an autonomous dental implant robotic system in dental implant surgery., Yu Wu , Shiqi Zou , Pin Lv , Xiao Wang , The Journal of prosthetic dentistry. Volume: 133, Issue: 3, 2025
STATEMENT OF PROBLEM
Autonomous dental implant robot systems (ADIRSs) have been marketed for dental implant surgery; however, research on their accuracy is limited.
PURPOSE
The purpose of this clinical study was to examine the accuracy of an ADIRS.
MATERIAL AND METHODS
Seventy-four participants with partial edentulism underwent implant surgery by using the ADIRS. Before surgery, a cone beam computed tomography (CBCT) scan was conducted, and its image data were fed into the ADIRS navigation and positioning system for iterative reconstruction and surgical path planning. After local anesthesia administration, area disinfection, and patient registration, the robot prepared the osteotomy and placed the implant under guidance of the navigation system. A postoperative CBCT scan was made to assess deviations between the planned and actual implant positions. The global coronal, apical, and angular deviations were measured and analyzed. A generalized linear mixed model (GLMM) was used to compare the differences in major outcome variables (α=.05).
RESULTS
All implant procedures were successfully carried out without any complications during surgery. A total of 86 implants were placed in 74 participants. The mean ±standard deviation global coronal deviation, global apical deviation, and angular deviation was 0.61 ±0.20 mm (95% CI: 0.23 to 1.0 mm), 0.79 ±0.32 mm (95% CI: 0.17 to 1.41 mm), and 2.56 ±1.10 degrees (95% CI: 0.42 to 4.70 degrees), respectively. The findings from the GLMM revealed that the implant region (premolar, molar; maxilla, mandible; left, right), implant length, and surgeon did not significantly impact accuracy (P>.05).
CONCLUSIONS
ADIRS showed high accuracy for implant placement because of the control of angular deviation and axial errors. The implant region, implant length, and surgeon had no significant influence on the accuracy of implant placement. Nevertheless, more clinical studies are required to support evidence-based clinical outcomes. Read More
6. Feasibility and accuracy of a task-autonomous robot for zygomatic implant placement., Huanze Deng , Jing Wang , Le Liu , Yanfeng Li , The Journal of prosthetic dentistry. Volume: , Issue: , 2023
STATEMENT OF PROBLEM
Zygomatic implants (ZIs) should be placed accurately as planned preoperatively to minimize complications and maximize the use of the remaining bone. Current digital techniques such as static guides and dynamic navigation are affected by human error; therefore, new techniques are required to improve the accuracy of ZI placement.
PURPOSE
The purpose of this clinical study was to assess the feasibility and accuracy of a task-autonomous robot for ZI placement.
MATERIAL AND METHODS
Patients indicated for ZI placement were enrolled, and an appropriate surgical positioning piece was selected based on the presence of natural teeth in the maxilla. Preoperative cone beam computed tomography (CBCT) scanning was performed with the surgical positioning piece, and virtual implant design and socket preparation procedures were initiated. Implant socket preparation and placement were automatically performed by the robot according to the preoperative plan under the supervision of the surgeon. Postoperative CBCT scanning was performed to evaluate deviations between the virtual and actual implants. All quantitative data were expressed as standardized descriptive statistics (mean, standard deviation, minimum, maximum, and 95% confidence interval [CI]). The Shapiro-Wilk test was used to assess the normal distribution of all variables (α=.05).
RESULTS
Six participants were enrolled, and 8 ZIs were inserted. No intraoperative or postoperative complications were observed. Robotic ZI placement showed a global coronal deviation of 0.97 mm (95% CI: 0.55 to 1.39 mm), a global apical deviation of 1.27 mm (95% CI: 0.71 to 1.83 mm), and an angular deviation of 1.48 degrees (95% CI: 0.97 to 2.00 degrees).
CONCLUSIONS
Task-autonomous robots can be used for ZI placement with satisfactory accuracy. Robotic ZI surgery can be an alternative to static guidance and dynamic navigation to improve the accuracy of implant placement. Read More
7. Accuracy and efficiency of robotic dental implant surgery with different human-robot interactions: An in vitro study., Zonghe Xu , Yanjun Xiao , Lin Zhou , Yanjun Lin , Endian Su , Jiang Chen , Dong Wu , Journal of dentistry. Volume: 137, Issue: , 2023
OBJECTIVES
This study aims to compare the surgical efficiency (preparation and operation time) and accuracy of implant placement between robots with different human-robot interactions.
METHODS
The implant robots were divided into three groups: semi-active robot (SR), active robot (AR) and passive robot (PR). Each robot placed two implants (#31 and #36) on a phantom, practising 10 times. The surgical efficiency and accuracy of implant placement were then evaluated.
RESULTS
Sixty implants were placed in 30 phantoms. The mean preparation times for the AR, PR and SR groups were 3.85 ± 0.17 min, 2.14 ± 0.06 mins and 1.65 ± 0.19 mins, respectively. The mean operation time of the PR group (3.76 ± 0.59 min) was shorter that of than the AR (4.89 ± 0.70 mins) and SR (4.59 ± 0.56 min) groups (all P < 0.001). The operation time of the AR group in the anterior region (4.47 ± 0.31 min) was longer than that of the SR group (4.07 ± 0.10 min) (P = 0.007). The mean coronal, apical and axial deviations of the PR group (0.40 ± 0.12 mm, 0.49 ± 0.13 mm, 0.96 ± 0.22°) were higher than those of the AR (0.23 ± 0.11 mm, 0.24 ± 0.11 mm, 0.54 ± 0.20 °) (all P < 0.001) and SR (0.31 ± 0.10 mm, 0.36 ± 0.12 mm, 0.43 ± 0.14 °) groups (P = 0.044, P = 0.002, and P < 0.001, respectively).
CONCLUSIONS
Human-robot interactions affect the efficiency of implant surgery. Active and semi-active robots show comparable implant accuracy. However, the implants placed by the passive robot show higher deviations.
CLINICAL SIGNIFICANCE
This in vitro study preliminarily demonstrates that implant placement is accurate when using implant robots with different human-robot interactions. However, different human-robot interactions have variable surgical efficiencies. Read More
8. Autonomous robotic surgery for zygomatic implant placement and immediately loaded implant-supported full-arch prosthesis: a preliminary research., Changjian Li , Menglin Wang , Huanze Deng , Shumao Li , Xinyu Fang , Yijie Liang , Xihua Ma , Yue Zhang , Yanfeng Li , International journal of implant dentistry. Volume: 9, Issue: 1, 2023
OBJECTIVES
A patient with extensive atrophy of the alveolar ridge in the posterior portion of the maxilla was selected to complete an experimental and clinical case of the robotic zygomatic implant to investigate the viability of an implant robotic system in clinical use.
METHODS
The preoperative digital information was collected, and the implantation position and personalized optimization marks needed for robot surgery were designed in advance in a repair-oriented way. The resin models and marks of the patient's maxilla and mandible are all printed in 3D. Custom-made special precision drills and handpiece holders for robotic zygomatic implants were used to perform model experiments and compare the accuracy of the robotic zygomatic implant group (implant length = 52.5 mm, n = 10) with the alveolar implant group (implant length = 18 mm, n = 20). Based on the results of extraoral experiments, a clinical case of robotic surgery for zygomatic implant placement and immediate loading of implant-supported full arch prosthesis was carried out.
RESULTS
In the model experiment, the zygomatic implant group reported an entry point error of 0.78 ± 0.34 mm, an exit point error of 0.80 ± 0.25 mm, and an angle error of 1.33 ± 0.41degrees. In comparison, the alveolar implant group (control group) reported an entry point error of 0.81 ± 0.24 mm, an exit point error of 0.86 ± 0.32 mm, and an angle error of 1.71 ± 0.71 degrees. There was no significant difference between the two groups (p > 0.05). In clinical cases, the average entry point error of two zygomatic implants is 0.83 mm, the average exit point error is 1.10 mm and the angle error is 1.46 degrees.
CONCLUSIONS
The preoperative planning and surgical procedures developed in this study provide enough accuracy for robotic zygomatic implant surgery, and the overall deviation is small, which is not affected by the lateral wall deviation of maxillary sinus. Read More