This Week in Dental Implants, we wanted to focus on the socket shield technique, particularly with reference to a new study which applied a modified version of the technique to delayed implant placement and surprisingly found it to be quite beneficial in several respects. 9. A case is shown below with the modified socket shield technique (with immediate placement), as developed by Han et al.
Introduction of the Socket Shield Technique
The socket shield technique (SST), first described by Hurzeler 1, involves the intentional retention of a section of the tooth root during immediate implant placement. This technique aims to preserve the buccal/proximal bone from resorption, which often occurs after tooth extraction. The retained root fragment acts as a shield, preserving the buccal bone and soft tissue architecture. By maintaining a portion of the root, the socket shield technique helps to stabilize the surrounding bone and soft tissues, potentially leading to better aesthetic outcomes and reduced post-extraction tissue alteration.
Variations of the Socket Shield Technique
Different variations and improvements over the original socket shield technique have been proposed. For example, Gluckman et al. 2,3 introduced Partial extraction therapy (PET) which introduced a more refined approach to preserving the alveolar ridge and minimizing post-extraction resorption. One of the key changes is the emphasis on the preparation of the socket shield to the bone crest, which is crucial for optimizing the integration of the retained root structure with the surrounding tissues. This preparation technique aims to support soft tissue infill, and if present, the gap between the implant and the buccal portion of the root should be grafted with particulate graft.
Other variations, such as those proposed by Siormpas and Mitsias 4,5 maintain that it is not necessary to graft the space. In fact, Siormpas and Mitsias renamed the original SST to the root membrane technique to emphasize the goal of preserving the periodontal ligament and the intentional retention of a section of the root is to act as a membrane that protects the surrounding bone and soft tissues.
Finally, with respect this post, it is important to note another variation introduced by Han et al. called the Modified Socket Shield Technique (see case below) 8. In the modified socket shield technique, the buccal portion of the root is retained, with the shield being 1.5 mm thick and the most coronal portion at the bone crest level. Immediate implants are placed without graft material in the gap between the implant and the shield.
Indications of the Socket Shield Technique
The socket shield technique is specifically indicated for use in anterior esthetic sites where preserving the buccal bone and soft tissue architecture is crucial for achieving optimal aesthetic outcomes. It is particularly beneficial in cases where immediate implant placement is planned following tooth extraction, as it helps to maintain the facial contour of the alveolar ridge and minimize post-extraction resorption.
While initially described for anterior sites, the technique has also been explored for use in molar sites, although managing post-extractive ridge changes in the posterior region remains a challenge. 6,7 The socket shield technique aims to offset these ridge changes by preserving the patient’s residual tissues at immediate implant sites.
Socket Shield Technique for Delayed Implantation?
While the socket shield technique was indicated for immediate implants, the question is whether it can help even in cases of delayed implantantion. That was the subject of a recent study 9, which concluded:
The modified socket shield technique with delayed implantation demonstrated superior maintenance of buccal bone plate height and ridge width, along with significantly higher primary implant stability, compared to spontaneously healed sockets. This approach is beneficial for maintaining ridge integrity when immediate implant placement is not planned.
Case Modified Socket Shield Technique
Case By: Chang-Hun Han et al. The Modified Socket Shield Technique., Chang-Hun Han , Kwang-Bum Park , Francesco Guido Mangano , The Journal of craniofacial surgery. Volume: 29, Issue: 8, 2018

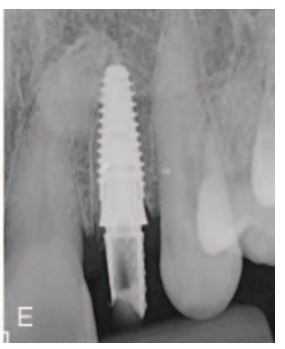
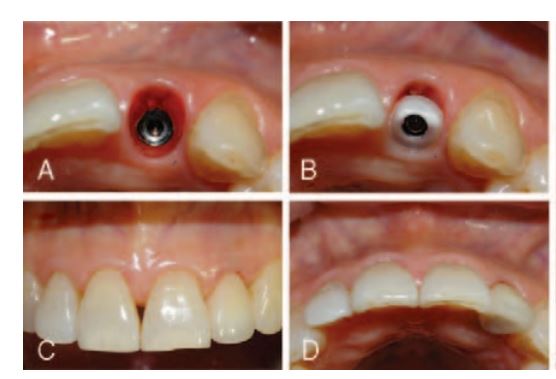
A 65-year-old female patient requested replacement of the left lateral incisor (No 22) due to a horizontal fracture: (A) preoperative situation, frontal view; (B) preoperative situation, occlusal view; (C) the root was sectioned and the lingual fragment was carefully removed. The remaining buccal fragment was thinned and concaved. After implant bed preparation, a tapered implant (AnyRidge) was inserted in contact with the retained root fragment; (D) a screw-retained provisional crown was fabricated and tightened onto the implant with 25 N/cm, the day after surgery; (E) postoperative periapical radiograph. Case By: Chang-Hun Han et al. The Modified Socket Shield Technique., Chang-Hun Han , Kwang-Bum Park , Francesco Guido Mangano , The Journal of craniofacial surgery. Volume: 29, Issue: 8, 2018

One week after surgery, the provisional restoration was removed (A) and the final impression was made. The definitive restoration consisted of a full zirconia abutment, tightened onto the implant using 30 N/cm of torque (B) and a full lithium disilicato crown (C, D), which was delivered after 2 weeks. A periapical radiograph was taken at the delivery of the final restoration (E). Case By: Chang-Hun Han et al. The Modified Socket Shield Technique., Chang-Hun Han , Kwang-Bum Park , Francesco Guido Mangano , The Journal of craniofacial surgery. Volume: 29, Issue: 8, 2018
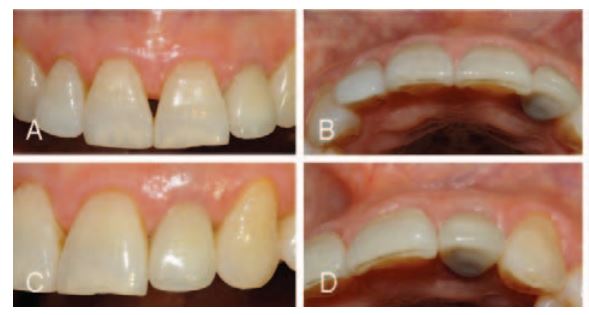
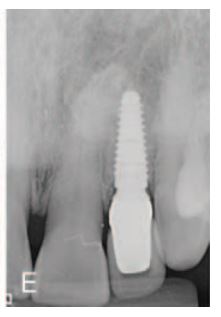
After 1 year of functional loading, the gingival architecture around the implant was well preserved, as evidenced from different views (A–D). The 1- year radiographic evaluation confirmed the stability of bone tissue around the implant (E). Case By: Chang-Hun Han et al. The Modified Socket Shield Technique., Chang-Hun Han , Kwang-Bum Park , Francesco Guido Mangano , The Journal of craniofacial surgery. Volume: 29, Issue: 8, 2018
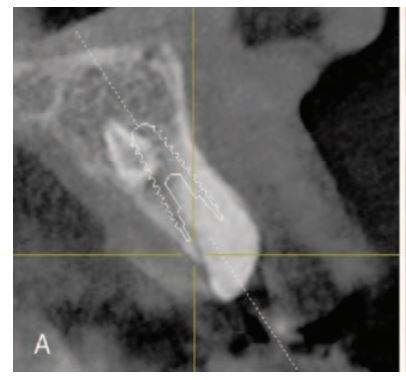
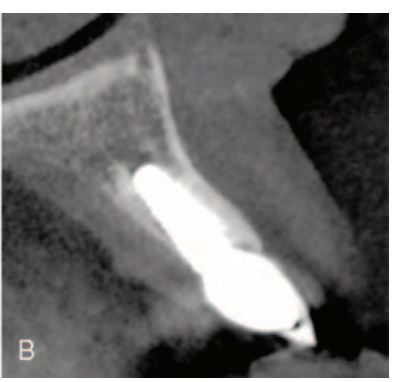
Preoperative (A) and 1-year follow-up control (B) CBCT. In the followup CBCT scan, shield is hardly distinguished from buccal bone plate. Periodontal ligament between shield and bone plate underwent atrophy. And even though fractured tooth did not have an endodontic treatment, shield and bone plate were well fused and look like cortical bone (corticalization). The implant was in contact with the shield. Case By: Chang-Hun Han et al. The Modified Socket Shield Technique., Chang-Hun Han , Kwang-Bum Park , Francesco Guido Mangano , The Journal of craniofacial surgery. Volume: 29, Issue: 8, 2018
Socket Shield Technique References
1. The socket-shield technique: a proof-of-principle report., Markus B Hürzeler , Otto Zuhr , Peter Schupbach , Stephan F Rebele , Notis Emmanouilidis , Stefan Fickl , Journal of clinical periodontology. Volume: 37, Issue: 9, 2010
AIM
Clinical studies have suggested that retaining roots of hopeless teeth may avoid tissue alterations after tooth extraction. Therefore, the objective of this proof-of-principle experiment was to histologically assess a partial root retention (socket-shield technique) in combination with immediate implant placement.
MATERIAL AND METHODS
In one beagle dog, the third and fourth mandibular pre-molar were hemisected and the buccal fragment of the distal root was retained approximately 1 mm coronal to the buccal bone plate. Following application of enamel matrix derivate, a titanium implant was placed lingual to that tooth fragment either with or without contact to the buccal tooth fragment and a healing abutment was connected. Four months after implant placement, histological evaluation, and backscatter scanning electron microscopy were performed.
RESULTS
All four implants were osseointegrated without any histologic inflammatory reaction and the tooth fragment was devoid of any resorptional processes. On the buccal side, the tooth fragment was attached to the buccal bone plate by a physiologic periodontal ligament. On the lingual side of the fragment, newly formed cementum could be detected. In the areas where the implant was placed into the fragment, newly formed cementum was demonstrated directly on the implant surface.
CONCLUSIONS
Retaining the buccal aspect of the root during implant placement does not appear to interfere with osseointegration and may be beneficial in preserving the buccal bone plate. Read More
2. Partial Extraction Therapies (PET) Part 1: Maintaining Alveolar Ridge Contour at Pontic and Immediate Implant Sites., Howard Gluckman , Maurice Salama , Jonathan Du Toit , The International journal of periodontics & restorative dentistry. Volume: 36, Issue: 5, 2016 Sep-Oct
Buccopalatal collapse of the postextraction ridge is a significant challenge in restorative and implant dentistry. A variety of ridge preservation techniques using tissue and augmentative materials have been proposed in the literature. A slightly different approach is to use the tooth itself. Root submergence has been reported in the literature for more than 4 decades, and it has been demonstrated that the submerged tooth root retains the periodontal tissues and preserves the bone in pontic sites or below dentures to retain the ridge. The socket-shield technique entails preparing a tooth root section simultaneous to immediate implant placement and has demonstrated histologic and clinical results that are highly promising to esthetic implant treatment. The pontic shield technique preserves the alveolar ridge at sites intended for pontic development where the root submergence technique is not possible. The aforementioned techniques collectively may be termed partial extraction therapies (PET), a term newly introduced into the literature and clinical environment. This article is a review of these ridge preservation therapies, providing a classification and a guide to their application. Read More3. Partial Extraction Therapies (PET) Part 2: Procedures and Technical Aspects., Howard Gluckman , Maurice Salama , Jonathan Du Toit , The International journal of periodontics & restorative dentistry. Volume: 37, Issue: 3, 2017 May/Jun
Part 1 of this series introduced the partial extraction therapies as a group of techniques for ridge preservation at immediate implant placement and beneath pontic sites. The concept proposes a paradigm shift away from extract and augment toward partly retaining the tooth root to preserve the ridge and prevent buccopalatal collapse. The revolutionary socket-shield technique was introduced in 2010; however, there has been no follow-up literature to guide the clinician in terms of procedural steps. While root submergence is well established, the socket-shield and pontic shield are still in their clinical infancy and require long-term clinical data before they can be proposed as routine in everyday implant dentistry. Yet without sound knowledge on how to carry out the partial extraction therapies, a global dental community cannot participate in their application or contribute to the growing knowledge base. In this, the second part of the series, the procedures for root submergence, socket-shield, and pontic shield are addressed, step by step, supplemented with applicable guidelines as the first such publication guiding the clinician to apply these root- and ridge-preservation techniques. Technical aspects and complication management are also addressed. Read More4. Immediate implant placement in the esthetic zone utilizing the "root-membrane" technique: clinical results up to 5 years postloading., Konstantinos D Siormpas , Miltiadis E Mitsias , Eleni Kontsiotou-Siormpa , David Garber , Georgios A Kotsakis , The International journal of oral & maxillofacial implants. Volume: 29, Issue: 6, 2014 Nov-Dec
PURPOSE
To clinically evaluate immediate implant placement with simultaneous intentional retention of the buccal aspect of the root and to report longitudinal data on survival of implants placed with the use of this novel technique.
MATERIALS AND METHODS
A retrospective case series of implants placed with the root-membrane technique in the maxillary anterior region of adult patients was conducted. Clinical and radiographic analysis was performed to assess implant success and to evaluate the survival of the retained root fragment based on predetermined criteria. A Kaplan-Meier method analysis was used to estimate the 5-year success rate of implants placed with this technique.
RESULTS
Data from 46 patients (median follow-up time, 40 months; range, 24 to 60 months) were evaluated. Each patient contributed one implant site in this study. All implants successfully maintained osseointegration at the end of the follow-up period for a 100% cumulative survival rate, based on clinical and radiographic criteria. Radiographic examination revealed good crestal bone stability with mean crestal bone loss on the mesial and distal aspects of the implants estimated to be 0.18 ± 0.09 mm and 0.21 ± 0.09 mm, respectively. The only complication noted in this patient cohort was apical root resorption of a single retained root fragment that did not interfere with the osseointegration of the implant.
CONCLUSION
The intentional retention of the buccal aspect of the root with its periodontal apparatus during immediate implant placement can lead to predictable and sustainable osseointegration of implants placed in the maxillary anterior region of healthy adults. Read More
5. A Step-by-Step Description of PDL-Mediated Ridge Preservation for Immediate Implant Rehabilitation in the Esthetic Region., Miltiadis E Mitsias , Konstantinos D Siormpas , Eleni Kontsiotou-Siormpa , Hari Prasad , David Garber , Georgios A Kotsakis , The International journal of periodontics & restorative dentistry. Volume: 35, Issue: 6, 2015 Nov-Dec
The aim of this study was to present in detail the clinical steps of the root-membrane technique. This technique combines the benefits of conventional root submergence via intentional maintenance of a root fragment for ridge preservation with those of immediate implant placement for functional rehabilitation of the treated site. A case study of a tooth diagnosed with a horizontal root fracture is used to illustrate this technique step by step. The clinical application of the root-membrane technique not only allowed for immediate placement in a site with compromised buccal plate but also facilitated excellent clinical stability of soft tissue contours during the 3 years of follow-up. Read More6. The socket-shield technique at molar sites: A proof-of-principle technique report., Charles W Schwimer , Howard Gluckman , Maurice Salama , Katalin Nagy , Jonathan Du Toit , The Journal of prosthetic dentistry. Volume: 121, Issue: 2, 2019
The socket-shield technique for avoiding postextraction tissue alteration was first described in 2010. The technique was developed for hopeless teeth in anterior esthetic sites but has not yet been described for molar sites. Managing postextractive ridge changes in the posterior region by prevention or regeneration remains a challenge. The socket shield aims to offset these ridge changes wherever possible, preserving the patient's residual tissues at immediate implants. This technique report describes the molar socket-shield step by step. Read More7. Evaluation of Healing at Molar Extraction Sites With and Without Ridge Preservation: A Randomized Controlled Clinical Trial., Christopher J Walker , Thomas J Prihoda , Brian L Mealey , David J Lasho , Marcel Noujeim , Guy Huynh-Ba , Journal of periodontology. Volume: 88, Issue: 3, 2017
BACKGROUND
To date, limited evidence is available specifically evaluating ridge preservation (RP) and implant placement in molar sites. The primary aim of this study is to radiographically compare alveolar ridge changes with and without RP with cone-beam computed tomography (CBCT).
METHODS
This parallel, two-arm randomized clinical trial included 40 patients evenly distributed between two treatment groups. After molar extraction, sites were allowed to heal naturally or received RP with freeze-dried bone allograft covered by a non-resorbable dense polytetrafluoroethylene membrane. CBCT scans were taken immediately and 3 months postextraction, and then a dental implant was placed. Width and height measurements were made radiographically.
RESULTS
Significantly greater loss in alveolar ridge height was found in molar sites allowed to heal without RP on the buccal aspect of the socket (RP: -1.12 ± 1.60 mm versus no RP: -2.60 ± 2.06 mm, P = 0.01). No significant difference in ridge width loss was found between groups. Two-thirds ridge width reduction was experienced on the buccal aspect in sites without RP, but width loss was evenly distributed between buccal and lingual aspects when RP was performed. Bone grafting at time of placement was required in 25% of implants in the group without RP versus 10% of implants in the RP group.
CONCLUSIONS
In molar extraction sites without RP, significantly more reduction in ridge height occurred, and the majority of ridge width loss was localized to the buccal aspect. When RP was performed, ridge width loss was not significantly decreased, but the loss was evenly distributed between facial and lingual aspects of the extraction site. Read More
8. The Modified Socket Shield Technique., Chang-Hun Han , Kwang-Bum Park , Francesco Guido Mangano , The Journal of craniofacial surgery. Volume: 29, Issue: 8, 2018
OBJECTIVE
In the anterior regions, the resorption of the buccal bone after tooth extraction leads to a contraction of the overlying soft tissues, resulting in an esthetic problem, particularly with immediate implant placement. In the socket shield technique, the buccal root section of the tooth is maintained, to preserve the buccal bone for immediate implant placement. The aim of this prospective study was to investigate the survival, stability, and complication rates of implants placed using a "modified" socket shield technique.
METHODS
Over a 2-year period, all patients referred to a dental clinic for treatment with oral implants were considered for inclusion in this study. Inclusion criteria were healthy adult patients who presented nonrestorable single teeth with intact buccal periodontal tissues in the anterior regions of both jaws. Exclusion criteria were teeth with present/past periodontal disease, vertical root fractures on the buccal aspect, horizontal fractures below bone level, and external/internal resorptions. The buccal portion of the root was retained to prevent the resorption of the buccal bone; the shield was 1.5 mm thick with the most coronal portion at the bone crest level. All patients then underwent immediate implants. In the patient with a gap between the implant and shield, no graft material was placed. All implants were immediately restored with single crowns and followed for 1 year. The main outcomes were implant survival, stability, and complications.
RESULTS
Thirty patients (15 males, 15 females; mean age was 48.2 ± 15.0 years) were enrolled in the study and installed with 40 immediate implants. After 1 year, all implants were functioning, for a survival rate of 100%; excellent implant stability was reported (mean implant stability quotient at placement: 72.9 ± 5.9; after 1 year: 74.6 ± 2.7). No biologic complications were reported, and the incidence of prosthetic complications was low (2.5%).
CONCLUSIONS
The "modified" socket shield technique seems to be a successful procedure when combined with immediate implant placement, because the root fragment does not interfere with osseointegration and may be beneficial for the esthetics, protecting the buccal bone from resorption. Read More
9. Dimensional Changes of Alveolar Ridge After Tooth Extraction Using the Socket Shield Technique Without Immediate Implant Placement: A Randomized Controlled Study., Soaad Tolba Badawy , The International journal of oral & maxillofacial implants. Volume: 0, Issue: 0, 2025
BACKGROUND
Alveolar ridge preservation is essential for successful implant placement and prosthetic rehabilitation. The modified socket shield technique (mSST) is one of the techniques developed to minimize ridge resorption.
OBJECTIVE
To compare radiographic dimensional changes in post-extraction sites treated with spontaneous healing versus the mSST without immediate implantation using cone beam computed tomography (CBCT). Study Design, Setting, Sample: This randomized clinical study included 80 patients with a singlenon-restorable non-molar maxillary tooth. Patients were divided into two equal groups: the test group (mSST) and the control group (atraumatic extraction with spontaneous healing). CBCT scans were performed at baseline (before or immediately after extraction) and 6 months post-surgery. Measurements included alveolar ridge width at 1 mm, 3 mm, and 5 mm levels, and buccal and palatal bone plate heights. Following this, implants were placed, and their primary stability was assessed.
INTERVENTION
The main intervention was the use of the mSST compared to atraumatic tooth extraction.
PRIMARY OUTCOME
included change in buccal bone plate height over a 6-month follow-up period. Covariates: included patient age and gender.
ANALYSES
Paired t-tests and independent t-tests were used to evaluate intra- and intergroup differences, respectively. Statistical significance was set at p < 0.05.
RESULTS
In the test group, a significant reduction in palatal wall height was observed (p < 0.001), while no significant changes were noted in other parameters (p ≥ 0.05). In the control group, significant decreases were seen in buccal and palatal plate heights and ridge width (p < 0.05). Comparing the groups, the test group demonstrated significantly less buccal wall height and ridge width resorption than the control group (p < 0.05). However, no significant difference was observed in palatal plate height resorption between groups (p = 0.507). The test group exhibited significantly higher primary stability compared to the control group (p = 0.001).
CONCLUSION AND RELEVANCE
The modified socket shield technique with delayed implantation demonstrated superior maintenance of buccal bone plate height and ridge width, along with significantly higher primary implant stability, compared to spontaneously healed sockets. This approach is beneficial for maintaining ridge integrity when immediate implant placement is not planned. Read More
10. The socket-shield technique: first histological, clinical, and volumetrical observations after separation of the buccal tooth segment – a pilot study., Daniel Bäumer , Otto Zuhr , Stephan Rebele , David Schneider , Peter Schupbach , Markus Hürzeler , Clinical implant dentistry and related research. Volume: 17, Issue: 1, 2015
BACKGROUND
The "socket-shield technique" has shown its potential in preserving buccal tissues. However, front teeth often have to be extracted due to vertical fractures in buccolingual direction. It has not yet been investigated if the socket-shield technique can only be used with intact roots or also works with a modified shield design referring to vertical fracture lines.
PURPOSE
The aim of this study was to assess histologically, clinically, and volumetrically the effect of separating the remaining buccal root segment in two pieces before immediate implant placement.
MATERIAL AND METHODS
Three beagle dogs were selected in the study. The third and fourth premolars on both sides of the upper jaw were hemisected and the clinical crown of the distal root was removed. Then, the implant bed preparation was performed into the distal root so that a buccal segment of healthy tooth structure remained. This segment was then separated in a vertical direction into two pieces and implants placed lingual to it. After 4 months of healing, the specimens were processed for histological diagnosis. In a clinical case, the same technique was applied and impressions taken for volumetric evaluation by digital superimposition.
RESULTS
The tooth segments showed healthy periodontal ligament on the buccal side. New bone was visible between implant surface and shield as well as inside the vertical drill line. No osteoclastic remodeling of the coronal part of the buccal plate was observed. The clinical volumetric analysis showed a mean loss of 0.88 mm in labial direction with a maximum of 1.67 mm and a minimum of 0.15 mm.
CONCLUSION
The applied modification seems not to interfere with implant osseointegration and may still preserve the buccal plate. It may offer a feasible treatment option for vertically fractured teeth. Read More
11. Clinical Benefits of the Immediate Implant Socket Shield Technique., Reza Saeidi Pour , Otto Zuhr , Markus Hürzeler , Otto Prandtner , Caroline Freitas Rafael , Daniel Edelhoff , Anja Liebermann , Journal of esthetic and restorative dentistry : official publication of the American Academy of Esthetic Dentistry ... [et al.]. Volume: 29, Issue: 2, 2017
OBJECTIVE
Extraction-socket resorption is considered a major problem that can limit implantological rehabilitation options and compromise the esthetic outcome. Surgical techniques to reduce remodeling are of restricted predictability and commonly require several surgical interventions and grafting. This increases the treatment cost and places a physical and psychological strain on the patient. This clinical case report presents a replacement of an upper canine using the socket-shield technique (SST) with a CAD/CAM surgical guide, resulting in a predictable, high esthetic, and functional result.
CLINICAL CONSIDERATIONS
The SST is an alternative approach to curbing remodeling and resorption by retaining the facial part of the root during tooth extraction. An immediately placed implant supports the facial root fragment, preventing the collapse of the buccal wall. The SST with digital precision planning in combination with a CAD/CAM surgical guide benefits patients by preserving their tissue architecture and causing only insignificant trauma. Furthermore, the SST reduces the number of surgical and prosthetic interventions required to one each for pre-operative planning, surgical procedures, and prosthetic rehabilitation.
CONCLUSIONS
The socket shield technique is a minimally invasive implantological approach offers patients and clinicians multiple benefits.
CLINICAL SIGNIFICANCE
The socket-shield technique (SST) represents an alternative approach to intervene remodeling and resorption processes by the maintenance of the facial part of the root during tooth extraction. The immediate placement of an implant supports the facial root fragment and thereby prevents a collapse of the buccal wall. The SST associated with a CAD/CAM fabricated surgical guide, can reduce the amount of appointments, due to the immediate fabrication of the definitive restoration with the existing model. Therefore, no further necessary appointments are required apart from first pre-operative planning, second for surgical treatment, and third for prosthetic rehabilitation. (J Esthet Restor Dent 29:93-101, 2017). Read More
12. Current Evidence on the Socket-Shield Technique: A Systematic Review., Amit S Gharpure , Neel B Bhatavadekar , The Journal of oral implantology. Volume: 43, Issue: 5, 2017
The recently popularized socket-shield technique involves intentional retention of a section of the remnant root at the time of immediate implant placement, thereby preserving the buccal/proximal bone from resorption. The objective of this systematic review was to assess the literature available on the socket-shield technique and weigh its biological plausibility and long-term clinical prognosis. A systematic search was performed on PubMed-Medline, Embase, Web of Knowledge, Google Scholar, and Cochrane Central for clinical/animal studies from January 1970 to April 2017. Twenty-three studies were assessed: 1 clinical case-control study, 4 animal histological reports, 1 clinical abstract, and 17+2* case reports. Eighteen out of the 23 studies had a duration of ≤12 months. A quality assessment of 5 studies (4 animal histologic and 1 clinical case-control) performed using the modified Animal Research: Reporting of In Vivo Experiments guidelines revealed that 4/5 studies had low scores. Fifty-eight out of 70 (82.86%) implants from 4 animal histological studies had complications; buccal/crestal bone loss (54.55%) and failure of osseointegration (27.27%) were the most common. Thirty-three out of 136 (24.26%) implants from 19+2 (2 studies had both histologic and clinical components, which are assessed separately) clinical studies had complications; buccal/crestal bone loss (78.78%) and shield exposure/failure (12.12%) were the most common. Other complications recorded were periodontal ligament and cementum formation on implant surfaces, pocket formation, inflammation, mucositis, and peri-implantitis. However, some clinical reports indicated stable results at 12 months. It would be difficult to predict the long-term success of this technique until high-quality evidence becomes available. A video abstract is available for viewing at https://youtu.be/lNMeUxj2XPA?list=PLvRxNhB9EJqbqjcYMbwKbwi8Xpbb0YuHI . Read More13. Socket Shield Technique for immediate implant placement - clinical, radiographic and volumetric data after 5 years., Daniel Bäumer , Otto Zuhr , Stephan Rebele , Markus Hürzeler , Clinical oral implants research. Volume: 28, Issue: 11, 2017
OBJECTIVES
Implant placement immediately after tooth extraction is often accompanied by resorption of surrounding tissues. A clinical technique was developed where the buccal portion of the root is retained to preserve the periodontal ligament and bundle bone. This technique is based on animal studies showing the potential to preserve the facial tissues utilizing this approach. The purpose of this study was to gain more insight regarding the safety of the technique with regard to biological and implant-related long-term complications and to observe the clinical appearance of the peri-implant tissues. Another objective was to evaluate volumetric changes of the affected facial contours in long-term and the esthetic outcomes.
MATERIAL AND METHODS
This study is a retrospective case series of 10 consecutive patients with implant replacement between the maxillary first premolars. Impressions were made prior to extraction (t1) and 5 years post-implant placement (t2). 3D-surface scans of the casts were digitally superimposed for quantitative evaluation of alterations of the facial peri-implant tissue contours and soft tissue recessions. Additionally, clinical data were collected (PPD, BOP, peri-apical radiographs and photographs).
RESULTS
All implants healed without adverse events. Peri-implant probing revealed healthy conditions. The comparison of radiographic images showed physiologic bone remodeling at the implant shoulders. Mean tissue loss on the facial side in oro-facial direction was -0.21 ± 0.18 mm. Average recession at implants was -0.33 ± 0.23 mm and at neighboring teeth -0.38 ± 0.27 mm. Mean loss of the marginal bone level at the implant shoulder amounted to 0.33 ± 0.43 mm at the mesial and 0.17 ± 0.36 mm at the distal aspect of the implants. A mean pink esthetic score of 12 was recorded.
CONCLUSION
Volumetric analysis showed a low degree of contour changes from extraction and implant placement to the follow-ups. Mucosal recession at the implant restoration was comparable to that of the neighboring teeth. Within the limitations of this descriptive study, the socket shield technique offers reduced invasiveness at the time of surgery and high esthetic outcomes with effective preservation of facial tissue contours. This technique should not be used in routine clinical practice until a higher level evidence in the form of prospective clinical trials is available. Read More