What role does the Keratinized mucosa (KM) width effect on peri‑implant disease? That is the subject of this review and case selection for This Week in Implants.
Quick Summary
Overall, while a sufficient band of keratinized mucosa (> 2 mm) may not be strictly required to prevent peri‑implant disease in well‑maintained patients, it does appear to reduce mucosal recession, lessen mucositis severity, and enhance the effectiveness of both non‑surgical and mechanical treatments. While the evidence is mixed, newer studies seem to show that a wider KM width should certainly be considered as a key factor influencing peri‑implant health and therapeutic outcomes.
Latest Study: The Role of the Keratinized Mucosa in Peri-Implant Diseases Onset and Brushing Discomfort: A 10-Year Follow-Up
This study was trying determine how the width of keratinized mucosa (KM) around dental implants (< 2 mm = narrow group, ≥ 2 mm = wide group) influences peri‑implant disease development and brushing discomfort over a ten‑year period. Clinical parameters (plaque indices, probing depth, clinical attachment level, mucosal recession, bleeding on probing, marginal bone level, brushing discomfort, and peri‑implant diagnosis) were recorded. At the 10‑year reassessment, 30 patients with 116 implants remained for analysis.
The study concluded:
A narrow KM favors plaque accumulation, mucosal recession, and peri-implant tissue inflammation in the long term, while a wider KM (≥ 2 mm) appears protective against peri-implant disease onset. Brushing discomfort declined over time irrespective of KM width. 1
Case: Keratinized Mucosa on the Risk of Peri‐Implant Diseases 20 Year Follow Up
This study evaluated 20‑year outcomes of tissue‑level implants placed in the posterior mandible, comparing implants surrounded by keratinized tissue (KT) with those surrounded by alveolar mucosa (AM). It concluded that: “Tissue level implants placed in the posterior mandible without KT showed greater marginal bone loss, bleeding on probing, soft tissue recession, and peri‐implant diseases compared to implants with KT at 20 years.” Thus, the presence of keratinized mucosa (or its augmentation via grafting) is associated with substantially better long‑term peri‑implant health in the posterior mandible. 2
Case photos below from: Roccuzzo A, Imber JC, Stähli A, Romandini M, Sculean A, Salvi GE, Roccuzzo M. [Role of Keratinized Mucosa on the Risk of Peri-Implant Diseases and Soft Tissue Dehiscence in the Posterior Mandible-A 20-Year Prospective Cohort Study.]
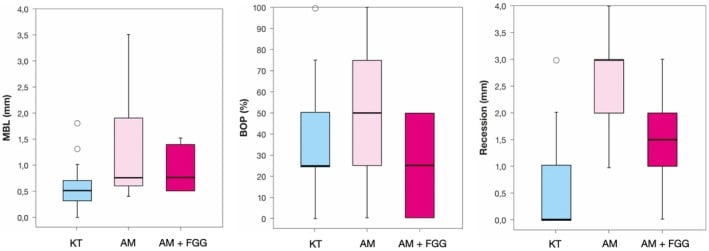
Box plots describing mean differences among the three groups (KT, keratinized tissue; AM, alveolar mucosa; AM + FGG, alveolar mucosa + free gingival graft) at the 20‐year examination with respect to the variables mean bone loss (MBL), bleeding on probing (BOP), and mucosal recession (REC).
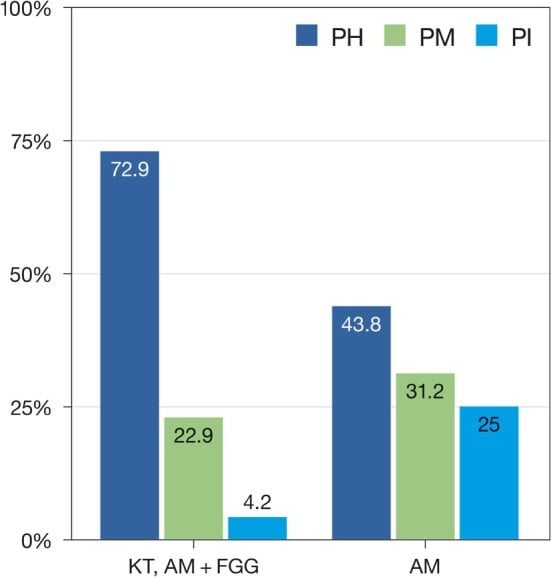
Peri‐implant conditions (i.e., peri‐implant health (PH), peri‐implant mucositis (PM) and peri‐implantitis (PI)) at the 20‐year examination with respect to the presence of keratinized tissue (i.e., KT, AM + FGG) or alveolar mucosa (AM).
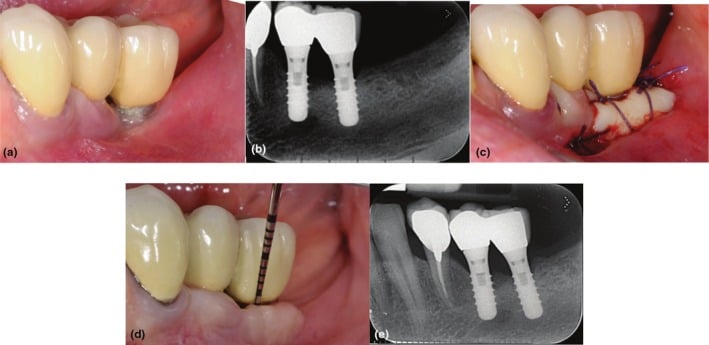
Clinical (a) and radiographic (b) views of the distal implant in region 3.6, placed 8 years earlier, demonstrate the lack of keratinized tissue (KT), peri‐implant soft‐tissue recession, and plaque accumulation. A free gingival graft (FGG) was performed to enhance the peri‐implant soft‐tissue conditions (c). Clinical (d) and radiographic (e) evaluations at the 20‐year follow‐up reveal minimal peri‐implant probing pocket depth, no bleeding on probing, and stable peri‐implant soft‐tissue conditions.
Case: The Significance of Keratinized Mucosa in Implant Therapy
In this case, a 65-year-old female with generalized periodontitis, stage IV grade C and very poor oral hygiene came for treatment and rehabilitation of the lower jaw. It concluded that: “There is insufficient knowledge in the literature regarding the correlation between inadequate KM and the occurrence of peri-implantitis. Further research in this area is needed, especially case–control studies, cohort studies and randomized clinical trials.”3
Case below by: Jankowski T, Jankowska A, Kazimierczak N, Kazimierczak W, Janiszewska-Olszowska J. [The Significance of Keratinized Mucosa in Implant Therapy: Narrative Literature Review and Case Report Presentation.](The Significance of Keratinized Mucosa in Implant Therapy: Narrative Literature Review and Case Report Presentation - PMC

Initial intraoral photographs: (A) right lateral view; (B) left lateral view; (C) frontal view.
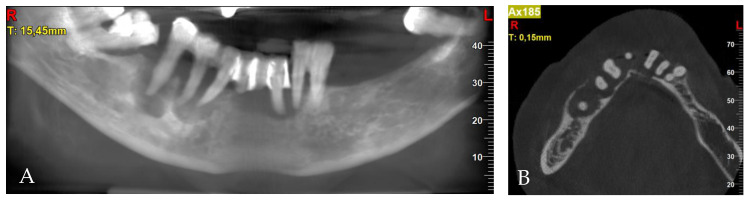
Pre-treatment CBCT: (A) panoramic view; (B) axial view; (C) cross-sections in position of teeth, respectively, 32; (D) 34; (E) 42; (F) 44; (G) 45; (H) 45.
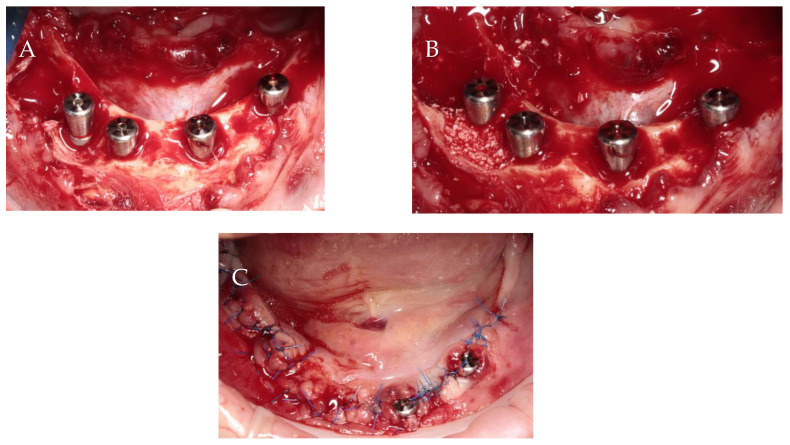
Surgical procedure: (A) implant insertion; (B) bone augmentation; (C) flap repositioning and suturing.
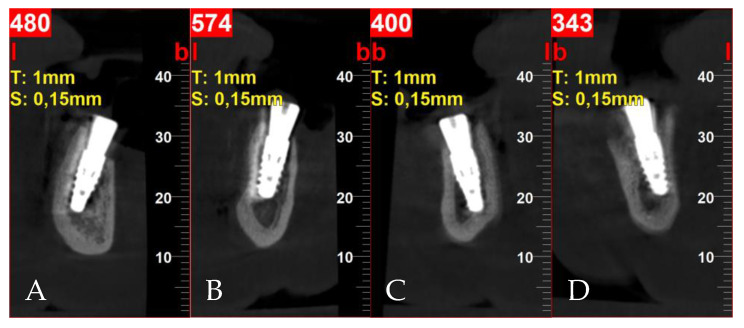
Postoperative cross-sectional CBCT scans: (A) tooth 32; (B) tooth 34; (C) tooth 42; (D) tooth 44.
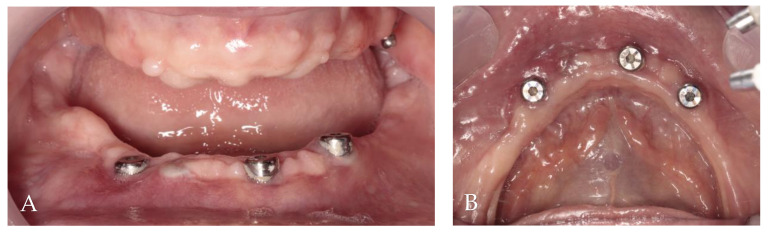
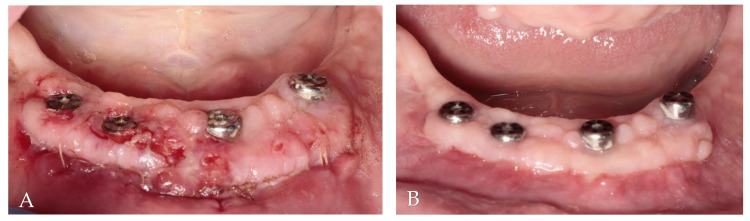
Two months post-op intraoral photographs: (A) frontal view; (B) occlusal view.
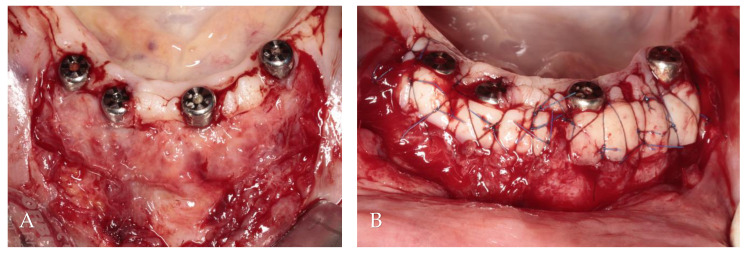
Soft tissue augmentation procedure: (A) preparation of the recipient site; (B) free gingival grafts stabilized by mattress sutures between residual KM and periosteum.
Clinical evaluation of soft tissue healing: (A) 2 weeks after augmentation; (B) 2 months after augmentation.
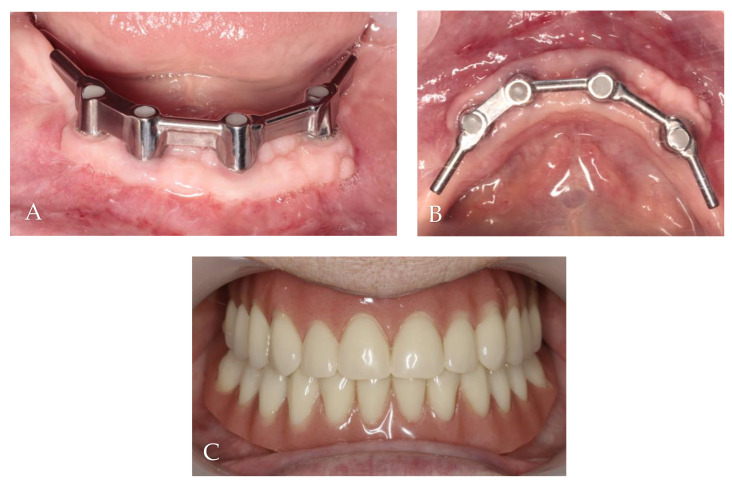
Follow-up clinical photographs: (A–C) 4 months after first surgery—the prosthetic restoration’s finalization; (D,E) 24 months after bar-retained overdenture delivery.
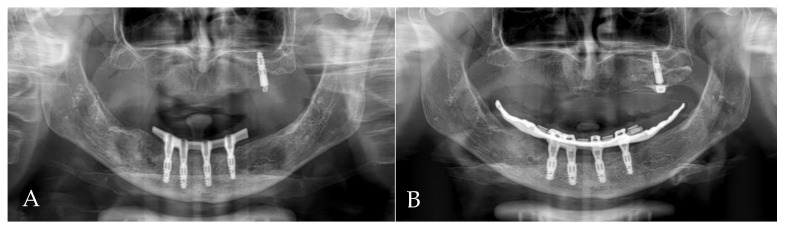
Orthopantomogram (OPG): (A) 4 months after first surgery—the prosthetic restoration’s finalization; (B) 24 months after bar-retained overdenture delivery.
Literature Review of Role of keratinized mucosa (KM) width in peri‑implant disease
| Evidence | Main finding about KM width | Clinical implication |
|---|---|---|
| Cross‑sectional study (231 implants) | KM < 2 mm was significantly associated with peri‑implant mucositis (OR ≈ 3.3) and with greater severity of the disease (mean difference ≈ 2.5 mm). | A narrow band of KM appears to be a risk indicator for developing and worsening mucositis. |
| Asian maintenance cohort (331 implants) | KM < 2 mm was linked to more mucosal recession (B = 0.12 mm). After adjusting for oral hygiene, smoking, periodontitis history and prosthesis type, plaque, inflammation and bone level were not related to KM width. | Insufficient KM may predispose to soft‑tissue recession, but not necessarily to plaque‑related inflammation or bone loss in well‑maintained patients. |
| Retrospective cohort (91 implants) | No statistically significant association between KM (≥ 2 mm vs < 2 mm) and either peri‑implant mucositis or peri‑implantitis (p ≥ 0.37). | In this sample, KM width did not influence disease prevalence. |
| 5‑year retrospective analysis (87 patients) | Correlations between KM width and disease parameters were negligible (‑0.2 < ρ < 0.2); no threshold width could be identified for health. | Suggests that, over the long term, the amount of KM is not a decisive factor for peri‑implant health in compliant patients. |
| Non‑surgical treatment of peri‑implantitis | After initial improvement, implants without KM showed a rebound increase in probing depth, bleeding on probing and plaque, whereas implants with KM maintained better outcomes. | Presence of KM supports better medium‑term response to non‑surgical therapy. |
| Prospective cohort on mucositis resolution | Narrow/absent KM (< 2 mm) reduced the odds of disease resolution by ≈ 80 % compared with wide KM (≥ 2 mm). Other clinical parameters also favoured the wide‑KM group. | Adequate KM enhances clinical resolution of mucositis after mechanical therapy. |
| Surgical treatment of peri‑implantitis | No difference in surgical outcomes (probing depth reduction, BOP, marginal bone gain) between KM < 2 mm and ≥ 2 mm groups; pre‑operative bone loss was the stronger predictor of survival. | KM width does not affect surgical success; bone status is more critical. |
Integrated summary
- Risk indicator: Several studies show that a KM width < 2 mm is associated with higher odds and greater severity of peri‑implant mucositis and with increased soft‑tissue recession.
- Disease prevalence: Other investigations (retrospective cohorts, 5‑year analysis) found no significant link between KM width and the occurrence of peri‑implant mucositis or peri‑implantitis.
- Treatment response: Both non‑surgical and mechanical‑therapy studies indicate that adequate KM (≥ 2 mm) improves the clinical response and stability after therapy, whereas lack of KM may lead to relapse of inflammation.
- Surgical outcomes: The amount of KM does not seem to influence the success of surgical management of peri‑implantitis; the severity of bone loss is more decisive.
References
-
da Costa Deller FA, Perussolo J, de Souza AB, de Oliveira RP, Matarazzo F, Araújo MG. The Role of the Keratinized Mucosa in Peri-Implant Diseases Onset and Brushing Discomfort: A 10-Year Follow-Up. Clin Oral Implants Res. 2026 Mar 29.
-
Roccuzzo A, Imber JC, Stähli A, Romandini M, Sculean A, Salvi GE, Roccuzzo M. Role of Keratinized Mucosa on the Risk of Peri-Implant Diseases and Soft Tissue Dehiscence in the Posterior Mandible-A 20-Year Prospective Cohort Study. J Periodontal Res.
-
Jankowski T, Jankowska A, Kazimierczak N, Kazimierczak W, Janiszewska-Olszowska J. The Significance of Keratinized Mucosa in Implant Therapy: Narrative Literature Review and Case Report Presentation. J Clin Med. 2024 Jun 14;13(12):3501.
-
The Effect of a Horizontal Apical Mattress Suturing Technique on the Width and Thickness of the Keratinized Mucosa After Dental Implant Surgery: A Cohort Study.
](The Effect of a Horizontal Apical Mattress Suturing Technique on the Width and Thickness of the Keratinized Mucosa After Dental Implant Surgery: A Cohort Study - PubMed) Tarek Khaled Abou-Agwa,Azzam Al-Jundi,Yasser Khaldoun Alhalaby,Hamzah Majed Alakari,Mohammad Y Hajeer et al., Cureus. Volume: 16, Issue: 7, 2024 -
Keratinized mucosa width is associated with severity of peri-implant mucositis. A cross-sectional study.
Jasmin Grischke,Annika Karch,Andreas Wenzlaff,Magdalena Marta Foitzik,Meike Stiesch,Jörg Eberhard et al., Clinical oral implants research. Volume: 30, Issue: 5, 2019 -
Peri-Implant Plastic Surgical Approaches to Increasing Keratinized Mucosa Width.
Esra Baltacıoğlu,Bora Bağış,Fatih Mehmet Korkmaz,Güven Aydın,Pınar Yuva,Yavuz Tolga Korkmaz et al., The Journal of oral implantology. Volume: 41, Issue: 3, 2015 -
Association between keratinized mucosa width and peri-implant diagnostic parameters in Asian maintenance compliers: A Cross-sectional study.
Sukuma Manopattanasoontorn,Kakanang Supanimitkul,Teerawut Tangsathian,Navawan Sophon,Sirikarn P Arunyanak,Kajorn Kungsadalpipob et al., Journal of the International Academy of Periodontology. Volume: 23, Issue: 2, 2021 -
Influence of keratinized mucosa on peri-implant diseases: a retrospective cohort study in humans.
Caroline Argolo Brito Oliveira,Vonei Luiz Pereira,Jean Nunes Dos Santos,Nara Santos Araujo,Patricia Ramos Cury et al., Oral and maxillofacial surgery. Volume: 28, Issue: 1, 2024 -
The Influence of Keratinized Mucosa on the Nonsurgical Therapeutic Treatment of Peri-Implantitis.
Carla Fons-Badal,Rubén Agustín-Panadero,Carlos Labaig-Rueda,Maria Fernanda Solá-Ruiz,Marina García-Selva,Antonio Fons Font et al., Journal of clinical medicine. Volume: 11, Issue: 14, 2022 -
The amount of keratinized mucosa may not influence peri-implant health in compliant patients: A retrospective 5-year analysis.
Hyun-Chang Lim,Daniel B Wiedemeier,Christoph H F Hämmerle,Daniel S Thoma et al., Journal of clinical periodontology. Volume: 46, Issue: 3, 2019 -
Influence of keratinized mucosa on the surgical therapeutical outcomes of peri-implantitis.
Andrea Ravidà,Islam Saleh,Rafael Siqueira,Carlos Garaicoa-Pazmiño,Muhammad H A Saleh,Alberto Monje,Hom-Lay Wang et al., Journal of clinical periodontology. Volume: 47, Issue: 4, 2020 -
Influence of keratinized mucosa width on the resolution of peri-implant mucositis: A prospective cohort study.
Gonzalo Blasi,Francesco Chierico,Ettore Amerio,Gerard Àlvarez,Sergio Isabal,Alexandre Arredondo,Vanessa Blanc,José Nart,Alberto Monje et al., Clinical implant dentistry and related research. Volume: 26, Issue: 3, 2024 -
Long-term evaluation of peri-implant keratinized mucosa stability after free epithelialized graft and keratinized mucosa shifting procedures: A retrospective study up to 13 years.
Ya-Chi Chen,Yu-Lin Lai,Jui-Ying Yen,Yi-Chun Lin,Hsuan-Hung Chen,Shyh-Yuan Lee et al., Clinical oral implants research. Volume: 34, Issue: 10, 2023 -
Keratinized mucosa width assessment at implant sites using high-frequency ultrasonography.
Lorenzo Tavelli,Ning Yu,Leonardo Mancini,Shayan Barootchi et al., Journal of periodontology. Volume: 94, Issue: 8, 2023 -
Efficacy of soft tissue substitutes, in comparison with autogenous grafts, in surgical procedures aiming to increase the peri-implant keratinized mucosa: A systematic review.
Eduardo Montero,Ana Molina,Paula Matesanz,Alberto Monje,Ignacio Sanz-Sánchez,David Herrera et al., Clinical oral implants research. Volume: 33 Suppl 23, Issue: , 2022