To achieve the best possible results during immediate implant placement choosing a proper flap design is a critical decision. A key consideration, is whether to raise a flap or not? Both techniques have benefits and drawbacks. This Week in Dental Implants we review some recent studies on this topic and highlight two interesting cases.
Latest Research: Impact of Soft-tissue Management techniques on Immediate Implant Placement: A Randomized Controlled Trial
A recent prospective randomized controlled trial with 46 patients receiving 48 implants compared the esthetic and tissue‑stability outcomes of open‑healing (flapless) versus closed‑healing (flap raised) techniques in immediate implant placement. The primary endpoint was the Pink Esthetic Score (PES),
Results
- Esthetic outcome: Open healing yielded significantly higher PES than closed healing (mean difference = ‑1.49; 95 % CI = [‑2.36, ‑0.62]; p = 0.0014).
- Higher baseline PES predicted better follow‑up esthetics (beta = 0.3638; p = 0.0002).
- Smoking showed no significant effect.
- Volumetric changes: Soft‑tissue volume decreased from T1 to T2 and partially recovered by T3. The open‑healing group experienced slightly less volume loss, but differences were not statistically significant.
- Implant survival: No implant loss in either group.
The study concluded:
Overall, the findings of this study contribute to the ongoing debate about the optimal healing technique for immediate implants and provide guidance for clinical decision making. While both methods appear effective in terms of implant survival, the esthetic advantages of the open healing technique, given the small differences in volumetric changes, may make it the preferred choice for patients and clinicians aiming for superior esthetic outcomes. These improved outcomes may be attributed to avoiding a flap elevation procedure and, therefore, periosteal elevation of the buccal implant wall, which may preserve buccal bone vascularization and therefore reduce the rate of bone resorption. 1
Additional Study: Flap versus Flapless Immediate Implants with Bone Augmentation: A Novel Study
Another earlier study compared traditional flap elevation with a flapless approach for immediate implant placement, with 60 patients randomly assigned to 2 groups. The study focused on bone healing and clinical success when bone augmentation is used, specifically measuring plaque index, wound‑healing index, crestal bone loss, and radiographic outcomes.
- Results
- Plaque indices improved in both groups.
- Modified gingival index showed improvement throughout healing.
- The flapless technique demonstrated superior crestal bone preservation.
- Conclusion
Within the constraints of this study, it can be said that this research demonstrated that augmentation procedures could successfully place implants in freshly extracted sockets with or without elevation of the mucoperiosteal flap. Flapless implantation offers a number of benefits, including shorter recovery times, reduced surgical hemorrhage, preservation of both soft and hard tissues, and patient comfort. 2
Related Cases
Case 1: Soft tissue dimensional change using customized titanium healing abutment in immediate implant placement in posterior teeth
Case photos below are from Soft tissue dimensional change using customized titanium healing abutment in immediate implant placement in posterior teeth.
Tanporn Lertwongpaisan,Parinya Amornsettachai,Woraphong Panyayong et al.,
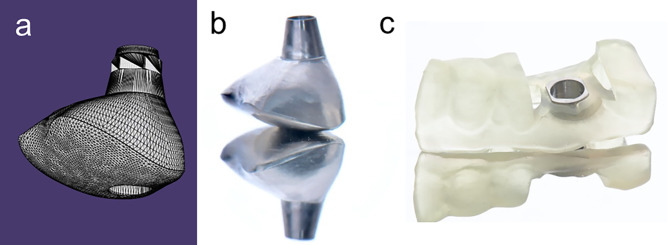
(a) The design of customization of healing abutment in form STL (Standard Triangle Language) file format, (b) The customized titanium healing abutment was milled from titanium blank, (c) The surgical template with a metal sleeve was designed following implantation plan.
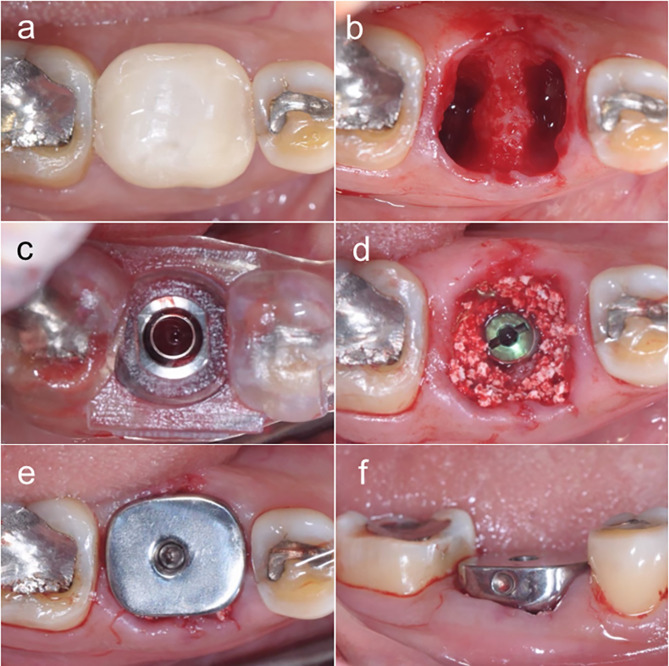
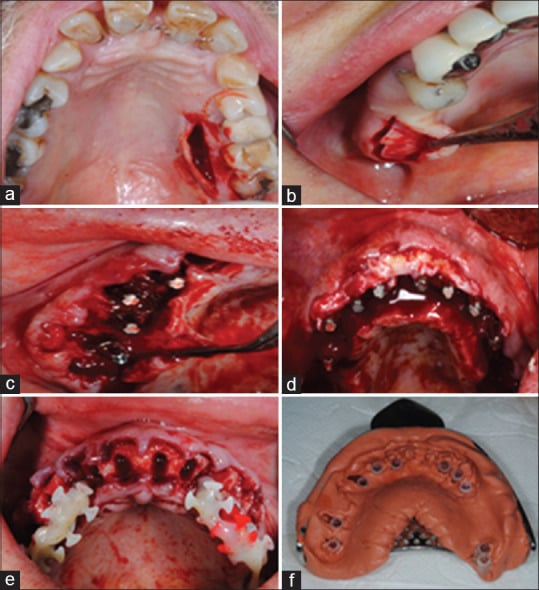
(a) Tooth #30 with inadequate restorative tooth structure, (b) Tooth #30 was extracted with minimal traumatic technique, (c) Complete implantation through a surgical template, (d) Alloplastic bone was grafted into the peri-implant gap, (e) occlusal view, (f) buccal view: The customized titanium healing abutment was connected to the implant fixture and seal on socket wound.
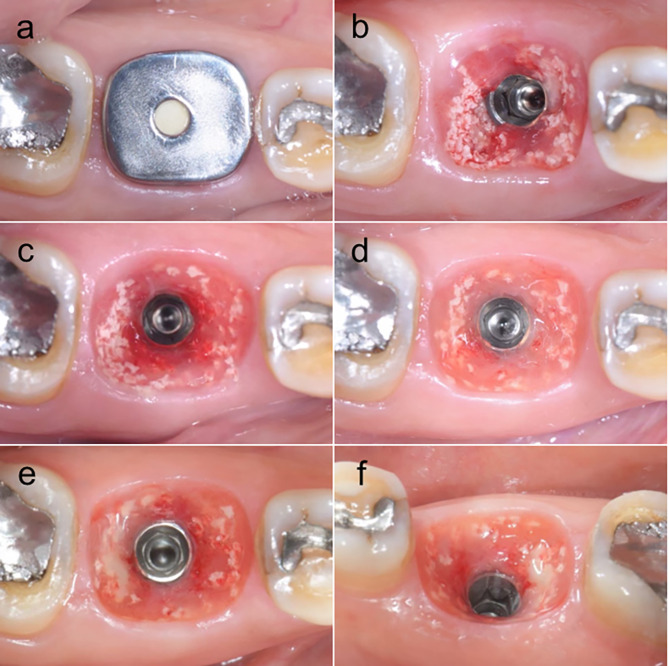
(a) The appearance of customized titanium healing abutment and peri-implant mucosa in each following time, (b) The peri-implant mucosa in 1st week follow-up, (c) The peri-implant mucosa in 1st month follow-up, (d) The peri-implant mucosa in 3rd months follow-up, (e) occlusal view, (f) lingual view: The peri-implant mucosa in 6th months follow-up
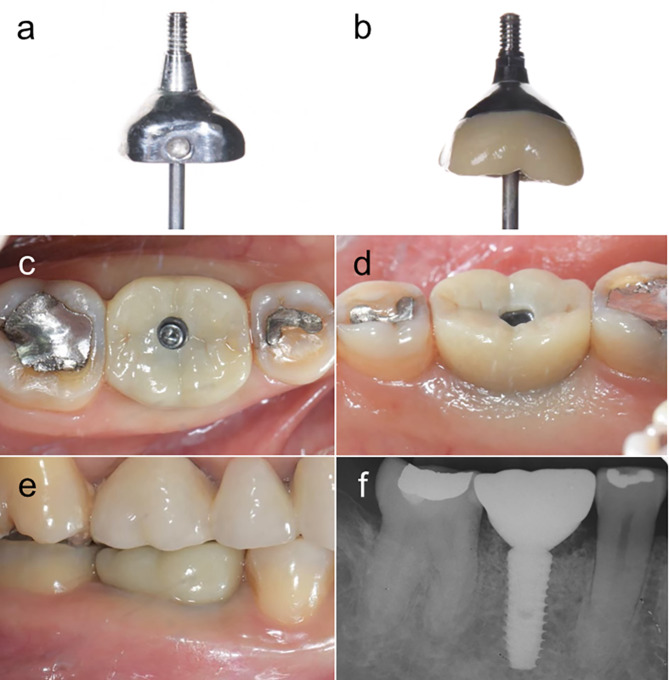
(a), (b) The outline form comparison between the customized titanium healing abutment and final prosthetic abutment with zirconia crown, (c) occlusal view, (d) lingual view, (e) buccal view, (f) radiographic examination: The final screw-retained implant prosthesis was complete after 6 months
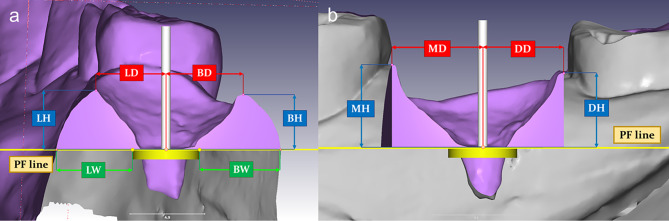
(a) Measurement in the buccal-lingual section, (b) Measurement in the mesial-distal section
Results
- Overall, the customized titanium healing abutments maintained optimal peri‑implant mucosa.
- No significant reduction was observed in margin distances and heights across intermittent periods.
- Cumulative reductions over the 6‑month follow‑up were:
- Margin height loss: Buccal 0.63 mm, Lingual 0.93 mm, Mesial 0.08 mm, Distal 0.24 mm.
- Contour‑width loss: Buccal 0.59 mm, Lingual 0.43 mm, Buccolingual 1.03 mm.
- A significant decrease was noted in total buccolingual contour width at 1 month and in total volume between the 3‑ and 6‑month visits.
Conclusion
Immediate implant placement combined with a customized titanium healing abutment effectively preserves peri‑implant soft‑tissue dimensions, offering a viable alternative for soft‑tissue management in posterior teeth. 3
Case 2: Soft-Tissue Augmentation in Periodontally Compromised Patients during Immediate Placement and Immediate Loading Dental Implant Surgery - A Retrospective Study
Case photos below by: Soft-Tissue Augmentation in Periodontally Compromised Patients during Immediate Placement and Immediate Loading Dental Implant Surgery - A Retrospective Study.
Aleksandar Lazarov et al.,
(a) A single-incision technique to minimise the donor site morbidity, (b) An abundance of soft tissue in the tuberosity area that should be removed for better positioning of the abutment head, (c) An abundance of palatine keratinised tissue after removing the granulation tissue and trimming the thin bony spicules, (d) A buccally repositioned de-epithelised palatal graft, (e) The impression is taken after the placement of the implants, before positioning the graft and suturing the flap, (f) Precise bone architecture is recorded to give proper orientation for the technician for marginal overcontouring of the bridge
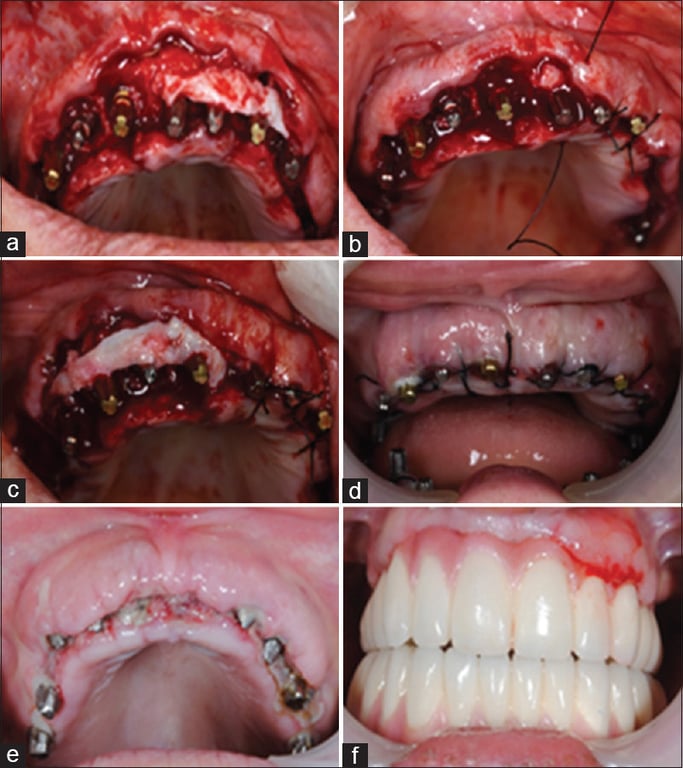
(a) The graft is positioned in a way to cover the buccal-marginal part of the abutments, (b and c) The buccal flap is released and coronally advanced to completely cover the graft, (d) Post-operative view of the grafted site, (e) 72-h post-operative appearance of the grafted site before cementation of the MFC restoration, (f) The graft 3 days after the cementation of the MFC bridge. MFC: Metal-fused-to-ceramic

(a-c) 1-year and 6-month post-operative appearance, showing a good adaptation of healthy augmented mucosa to the margins of the prosthesis

Gum recession around tooth number 25, revealing metal exposure and gap formation
Results
- Extent of grafting:
- 56.60 % of the 53 CTG patients had six, seven, or eight tooth sites grafted.
- 87 % needed CTGs at the canine teeth (teeth 13 and 23) (p < 0.001).
- Gum recession:
- Overall low recession rates in both groups.
- Significantly lower recession at tooth 13 in the CTG group (2.20 % vs. 18 %; p = 0.016).
- Across the ten tooth sites receiving CTGs, recession was also significantly reduced (p = 0.001).
- Patient satisfaction: 100 % of CTG patients reported reduced gum problems and greater satisfaction with gum health and aesthetics.
Discussion & Conclusions
Soft‑tissue augmentation with CTGs at multiple extraction sites during IPIL implant treatment appears to:
- Enhance the prosthesis‑tissue interface in aesthetic zones.
- Decrease gum infections, swelling, bleeding, and pain.
- Provide better aesthetic outcomes and patient satisfaction.
Thus, incorporating CTGs into immediate implant placement and loading protocols can be beneficial for periodontally compromised patients. 4
References
-
[Impact of soft-tissue management techniques on immediate implant placement: a randomized controlled trial.] (Impact of soft-tissue management techniques on immediate implant placement: a randomized controlled trial - PMC)
Frederic Bouffleur,Andreas Ruoss,Reinald Kühle et al., International journal of implant dentistry. Volume: 12, Issue: 1, 2026 -
Flap versus Flapless Immediate Implants with Bone Augmentation: A Novel Study.
Deepak Choudhary,Gaurav Girdhar,Santosh Kumar et al., Journal of pharmacy & bioallied sciences. Volume: 15, Issue: Suppl 2, 2023 -
Soft tissue dimensional change using customized titanium healing abutment in immediate implant placement in posterior teeth.
Tanporn Lertwongpaisan,Parinya Amornsettachai,Woraphong Panyayong et al., BMC oral health. Volume: 23, Issue: 1, 2023 -
Soft-Tissue Augmentation in Periodontally Compromised Patients during Immediate Placement and Immediate Loading Dental Implant Surgery - A Retrospective Study.
Aleksandar Lazarov et al., Annals of maxillofacial surgery. Volume: 13, Issue: 1, 2023 Jan-Jun