This Week in Dental Implants we wanted to do a quick review of the Cortical Shell Technique, demonstrating how it can be used to improve vertical and horizontal bone gains, particularly when used with computer-guided surgery as shown in a recent study. For further study, please use the references at the bottom of the page.
What is the Cortical Shell Technique?
The Cortical shell technique, popularized by Khoury, is a guided‑bone‑regeneration method in which a thin cortical bone plate (either harvested from the patient’s own mandible or obtained as an allogeneic cortical plate) is shaped and fixed to the defect site to act as a “shell” or container.
The shell is secured to the residual alveolar bone with miniscrews or a surgical template.
The space created between the shell and the host bone is then filled with particulate graft material (autogenous bone chips, allogeneic granules, xenografts or a mixture).
The shell serves as a scaffold that promotes vascular ingrowth and new bone formation within the contained space. As the grafted area is allowed to heal, new bone forms within the protected space, providing horizontal (and sometimes vertical) bone gain suitable for implant placement.
The technique can be performed free‑hand or, with computer‑guided workflows that use patient‑specific cutting and positioning guides to improve accuracy and predictability. It aims to avoid a second surgical site when allogeneic plates are used and to minimize donor‑site morbidity while achieving sufficient bone remodeling and stability.
Computer-guided Surgery vs Free Hand for the Cortical Shell Technique
Before getting to some cases, we wanted to call attention to a new study,
Computer-guided Versus Conventional Modified Cortical Shell Technique for the Rehabilitation of Posterior Mandibular Deficiency: Randomized Controlled Trial.
, that compared the horizontal bone gain and neurosensory function of a modified free- hand and a computer-guided cortical shell graft. The study concluded that:
The digital workflow of the modified cortical shell harvest, positioning and fixation enabled precise graft harvest and orientation, with a statistically significant horizontal bone gain exceeding that of the free-hand technique. 1
Cases: Allogeneic shell technique for alveolar ridge augmentation
Cases below by: Peer W Kämmerer,Jochen Tunkel,Werner Götz et al. The allogeneic shell technique for alveolar ridge augmentation: a multicenter case series and experiences of more than 300 cases. , International journal of implant dentistry. Volume: 8, Issue: 1, 2022
The shell technique is appropriate for alveolar ridge augmentation with adequate bone remodeling and low complication rates. Allografts can prevent donor site morbidity and therefore may decrease discomfort for the patient.
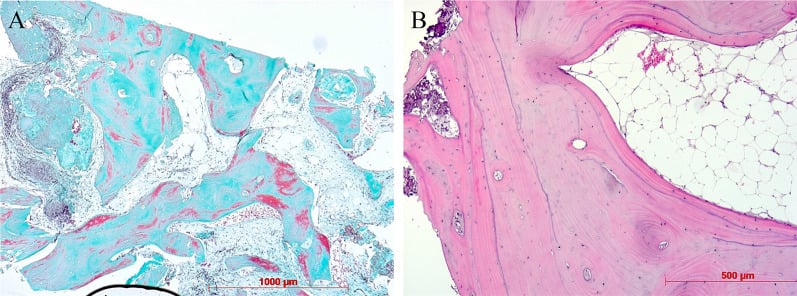
Fig. 1.
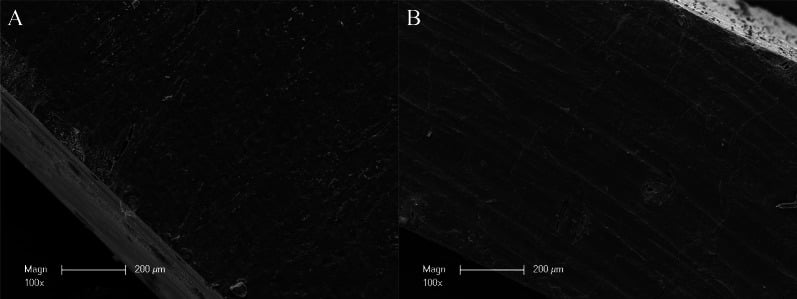
Overview about the microscopic structure and architecture of A the surface and B the side of an allogeneic cortical bone plate by scanning electron microscopy (SEM) at 100-fold magnification. SEM demonstrating the compact structure of allogeneic cortical bone plate that is suitable for a sufficient barrier and stabilization function
Fig. 2.
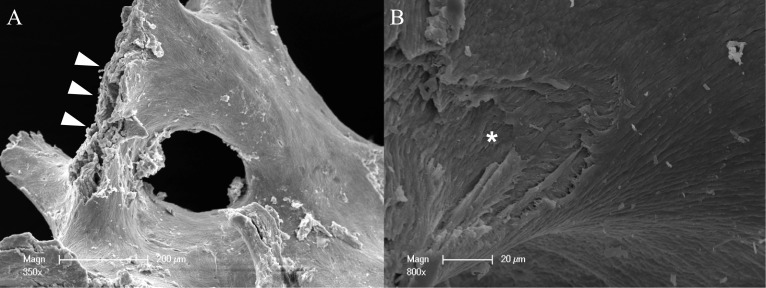
Overview about the microscopic structure and architecture of allogeneic spongious granules by scanning electron microscopy (SEM) in A low (350-fold) and B high (800-fold) magnification. A Allogeneic bone compositions consist of about 5% water and 30% collagen that is visible by the fan-shaped spreading edges (white arrows) and B by a multi-layered structure created by collagen fibers (white asterisk). SEM is even highlighting the porous structure of allogeneic spongious granules that is suitable for fast and sufficient micro-vessel ingrowth and bone remodeling.
Fig. 3.
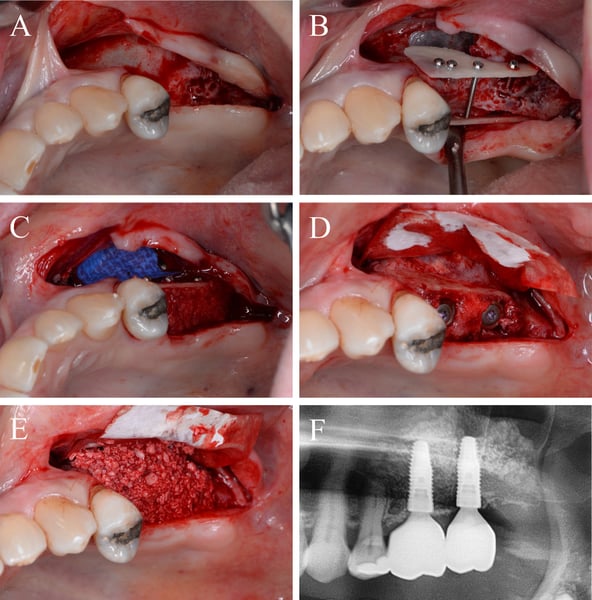
Alveolar ridge augmentation of the posterior maxilla. A Initial intraoperative situation with an extended alveolar defect of the posterior alveolar jaw. B Intraoperative situation after sinus floor elevation and fixation of two allogeneic cortical bone plates buccal and palatinal using four fixation screws. C Intraoperative situation after filling sinus floor with xenogeneic bone substitute, covering it with PTFE matrix and filling the alveolar crest with allogeneic spongious granules. D After 4 months, sufficient bone remodeling, screws removed, and implants inserted. E Overlining with xenogeneic granules for resorption protection and covered by collagen matrix. F X-ray demonstrating inserted implants.
Fig. 4.
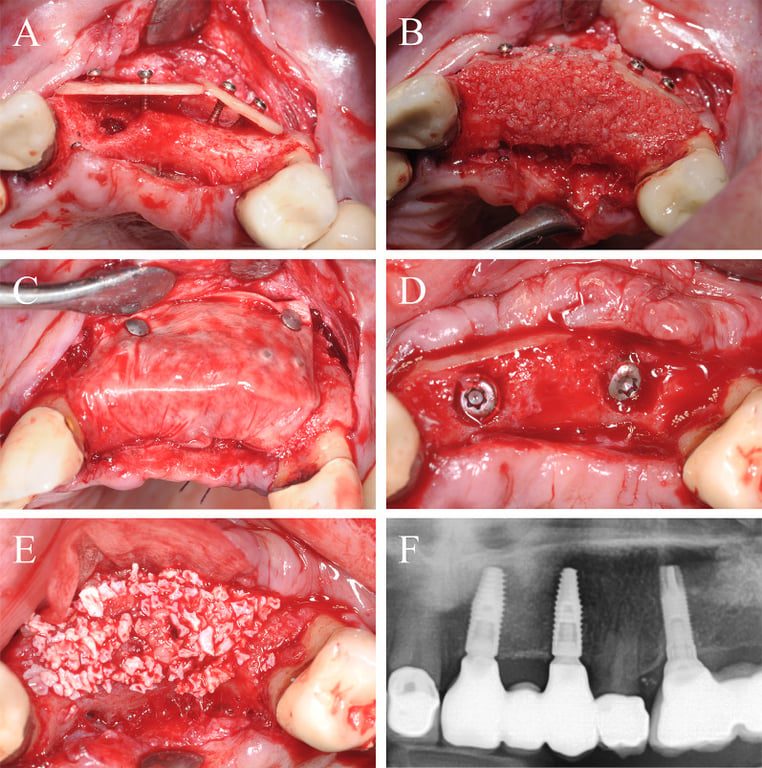
Alveolar ridge augmentation of the anterior maxilla. A Initial intraoperative situation with an extended alveolar defect of the anterior alveolar jaw. Two allogeneic cortical bone plates were fixed by fixation screws. B Intraoperative situation after filling the defect with allogeneic spongious granules. C Covering the augmented area with a porcine collagen membrane. D Implant placement 4 months later. E Overlining with xenogeneic bone graft to preserve the volume of the augmented area. F X-ray demonstrating inserted implants
Fig. 5.
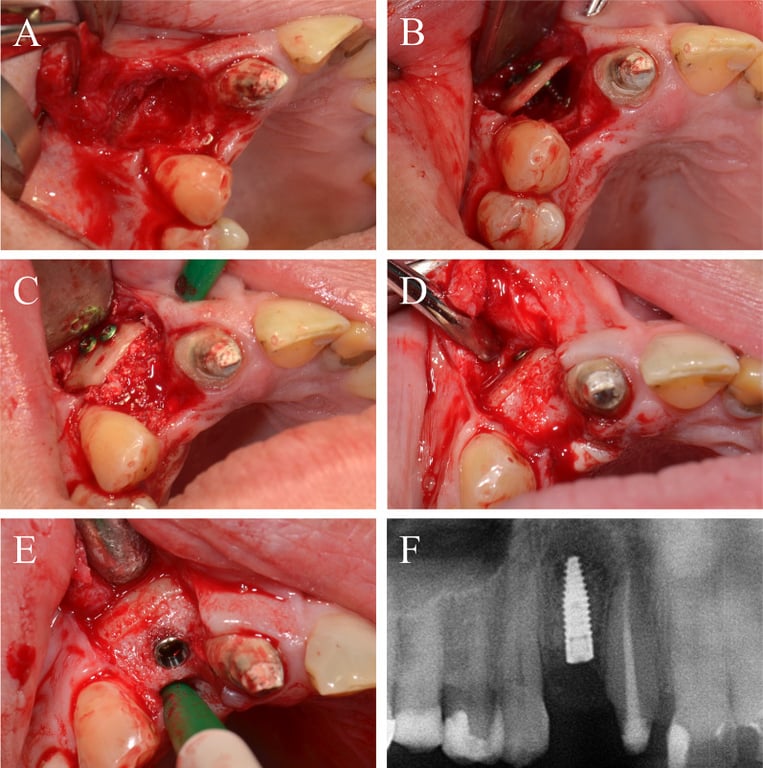
Alveolar ridge augmentation of the anterior maxilla. A Initial intraoperative situation demonstrating an extended tub-shaped alveolar defect after a failed augmentation attempt using an autogenous graft from the mandibular angle and postoperative hypesthesia of the mandibular nerve. B An allogeneic cortical bone plate was placed and fixed by adjusting screws. C The occurred space was filled with allogeneic spongious granules. D Four months later, a sufficient bone bed was found and E a bone level tapered implant was inserted. F X-ray demonstrating the inserted implant
Fig. 6.
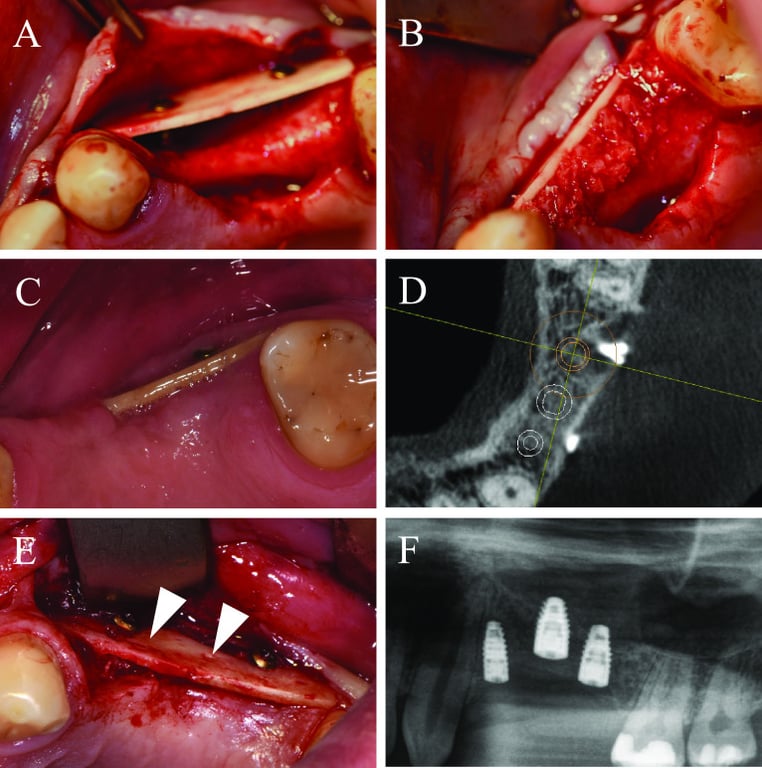
Alveolar ridge augmentation of the maxilla with wound dehiscence. A The intraoperative baseline showed an extended horizontal alveolar ridge atrophy. An allogeneic cortical bone plate was fixed laterally to the defect by two adjusting screws. B The space between the allogeneic cortical bone plate and the local alveolar ridge bone was filled with spongious allogeneic granules and the area was covered by a porcine pericardial matrix. C After a few weeks, a dehiscence defect with an exposure of the allogeneic CP was found. D Surgical re-evaluation demonstrated a plate fracture along the screw holes (white arrows). E CBCT scan demonstrated a sufficient bone volume for implant placement. F X-ray demonstrating the inserted implants
Fig. 7.
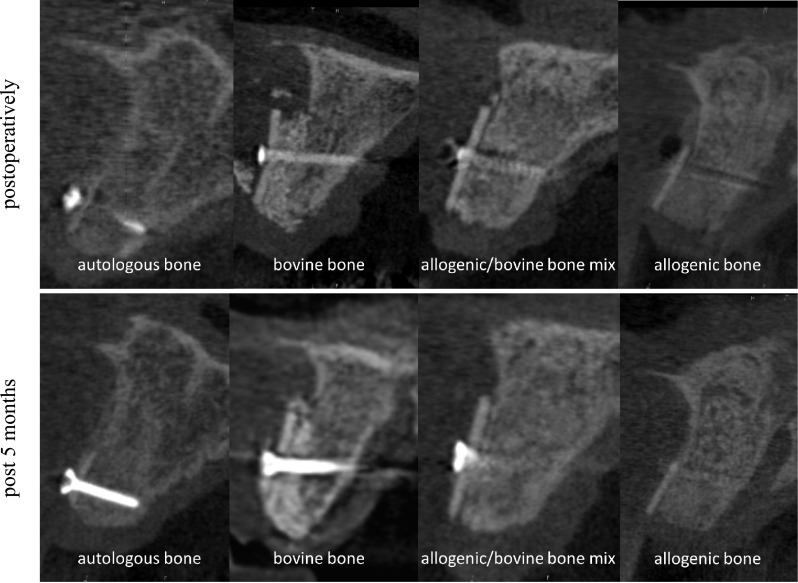
Alveolar ridge augmentation with different fillings, autologous bone, bovine substitute, a mixture of allogeneic bone and bovine substitute, and allogeneic bone at CBCT scans. Upper line situation postoperatively and lower line situation after 5 months in CBCT scans
Fig. 8.
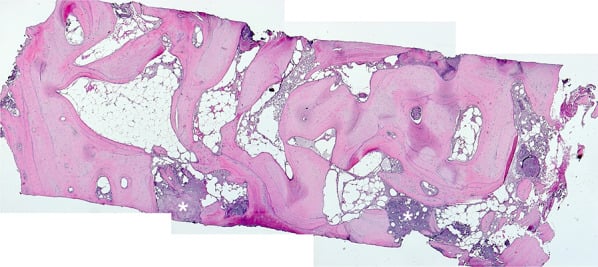
Overview after reconstruction of single sections, newly formed cancellous bone, white asterisks = detritus, HE staining, original magnification × 5
Fig. 9.
Newly formed cancellous bone, intertrabecular loose connective tissue, trichrome staining, original magnification × 5 (A). Newly formed cancellous lamellar bone, HE staining, original magnification × 10 (B)
Fig. 10.
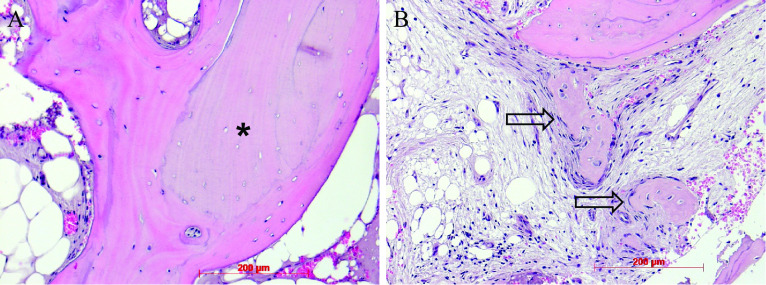
Newly formed cancellous lamellar bone, embedded allogenous remnant (black asterisk), HE staining, original magnification × 20 (A). Ongoing membranaceous osteogenesis, osteoblast covering (arrows), HE staining, original magnification × 20 (B)
Case: Alveolar ridge augmentation using the shell technique
Case below by: Jochen Tunkel,Luca de Stavola,Anita Kloss-Brandstätter et al., Clinical case reports. Volume: 9, Issue: 2, 2021 Alveolar ridge augmentation using the shell technique with allogeneic and autogenous bone plates in a split-mouth design-A retrospective case report from five patients.
This clinical case series emphasized that by means of the shell technique equal horizontal and vertical bone gain with both autogenous and allogeneic bone plates is achievable. The additional implementation of augmentative relining with a xenogeneic bone substitute material and collagen membrane seemed to minimize resorption processes and to maintain bone volume in the long term. However, this observation needs further replication in larger studies including a control group without relining.
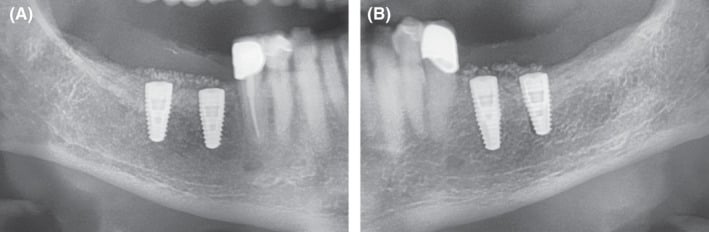
Figure 1.
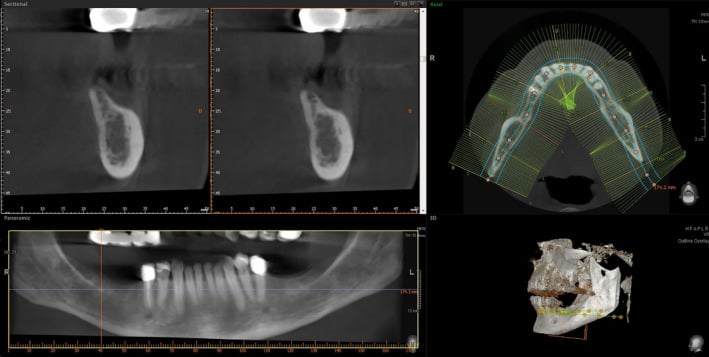
Preoperative CBCT: vertical bone defects in the third and fourth quadrant
Figure 2.
Augmentation in the third quadrant with autogenous bone plates and autogenous bone chips using the shell technique. A, horizontal and vertical defect in the third quadrant after flap elevation. B, buccal and lingual autologous bone plates fixed with microscrews utilizing the shell technique. C, bony envelope filled with autologous bone chips collected during thinning process of the bone plates
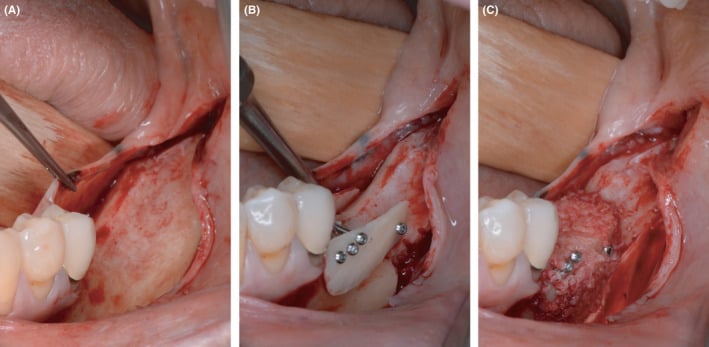
Figure 3.
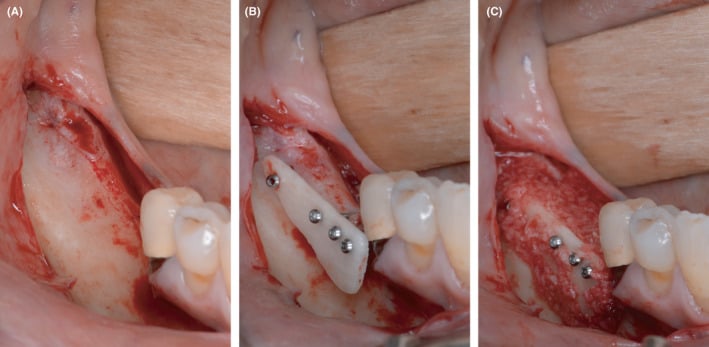
Augmentation in the fourth quadrant with allogeneic bone plates and autogenous bone chips using the shell technique. A, horizontal and vertical defect in the contralateral quadrant after flap elevation. B, buccal and lingual allogeneic bone plates fixed with microscrews utilizing the shell technique. C, bony envelope filled with autologous bone chips collected during thinning process of the autologous bone plates harvested in the third quadrant
Figure 4.
CBCT before implantation: significant vertical bone gain after 4 months of healing in both quadrants
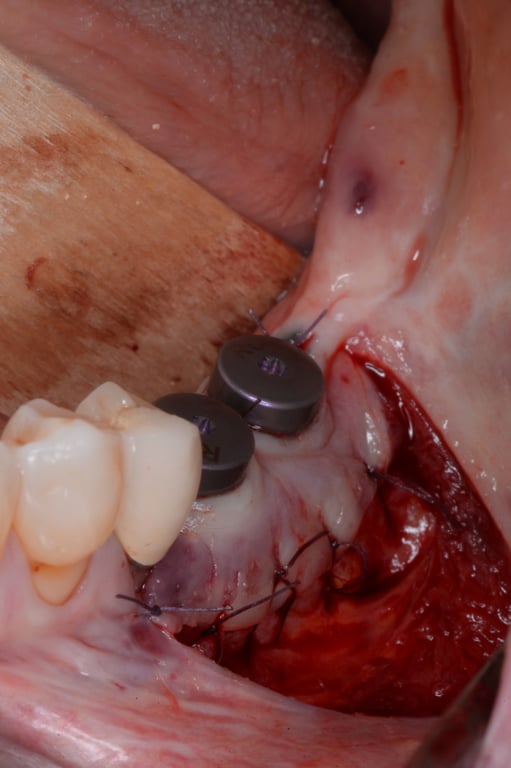
Figure 5.
Implantation in the third quadrant and augmentative relining with bovine bone substitute material and collagen membrane.A, regenerated bone of the autologous bone plate site with only minor signs of resorption. B, situation after insertion of two bone level implants and fixation of a collagen membrane for the relining GBR. C, relining process finished with DBBM particles and membrane stabilized by resorbable sutures
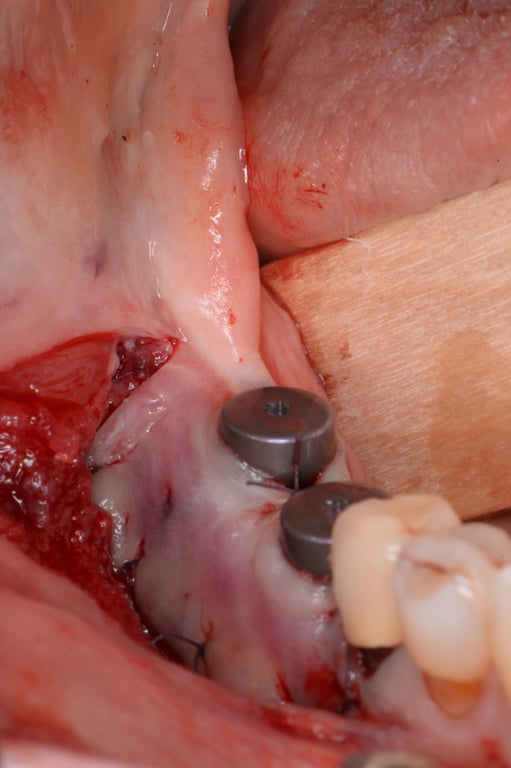
Figure 6.
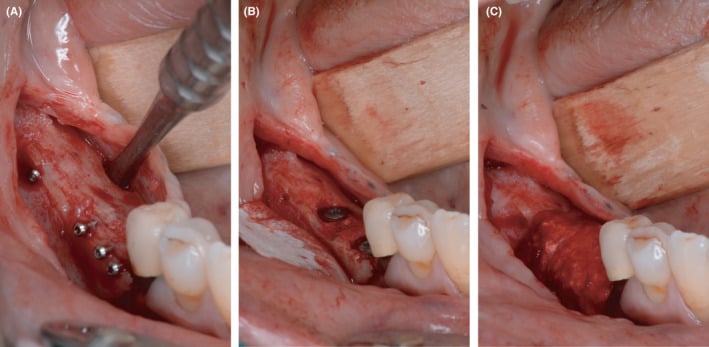
Implantation in the fourth quadrant and augmentative relining with bovine bone substitution material and collagen membrane. A, regenerated bone in the allogeneic bone plate site with only minor signs of resorption, as well. B, situation after insertion of two bone level implants and fixation of a collagen membrane for the relining GBR. C, relining process finished with DBBM particles and membrane stabilized by resorbable sutures
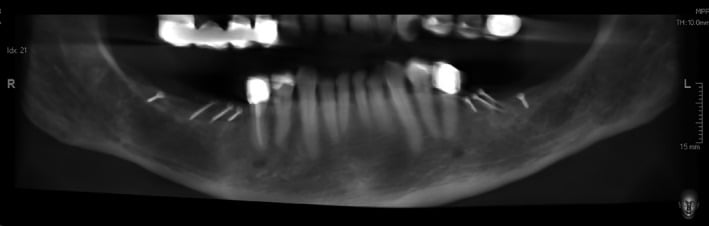
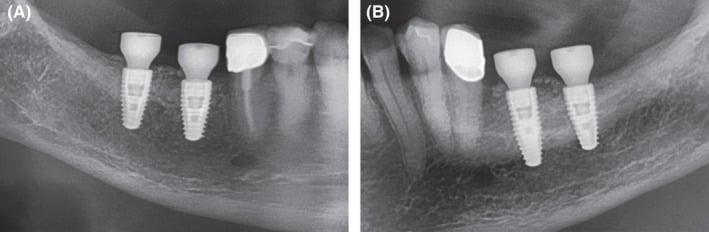
Figure 7.
Extracts from postoperative OPG after implantation and GBR in the third and fourth quadrant. A, fourth quadrant. B, third quadrant
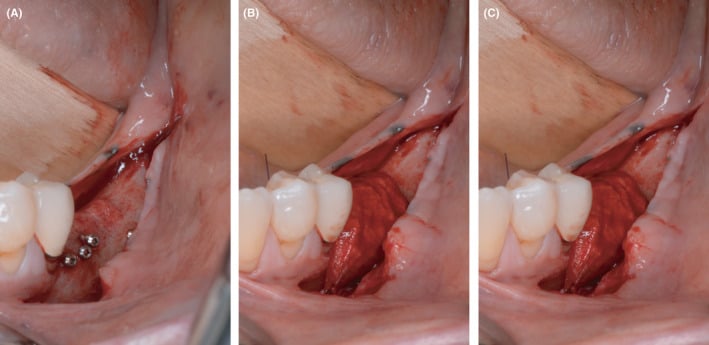
Figure 8.
Exposure of the implants in the third quadrant by stab incision combined with vestibuloplasty according to Kazanjian
Figure 9.
Exposure of the implants in the fourth quadrant by stab incision combined with vestibuloplasty according to Kazanjian
Figure 10.
Extracts from postoperative OPG: Gingival former in the third and fourth quadrants in situ. A, Allogeneic site showing good integration of the implants and no loss of crestal bone. Relining layer of DBBM particles in situ. B, Same situation on the autologous site showing similar results compared to the allogeneic site
Figure 11.
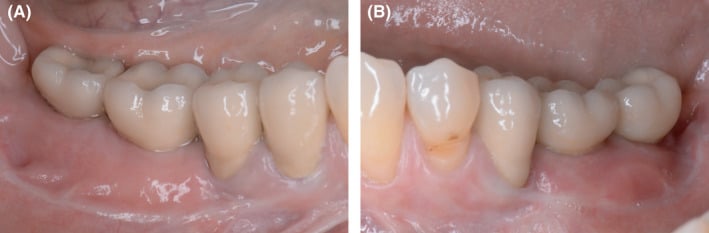
Clinical situation after prosthetic treatment in the third and fourth quadrant. A, Clinical result on the allogeneic site after prosthetics. Fixed mucosa was increased by Kazanjian vestibuloplasty to 5‐6mm. B, Similar clinical situation on the autologous bone plates site
Figure 12.
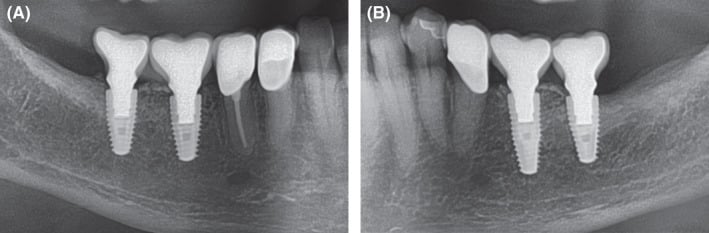
Extracts from OPG: Radiological situation after prosthetic treatment. A, Allogeneic site with good integration of the implants and no crestal bone loss and well‐integrated relining layer. B, Autologous site showing good integration, no bone loss and well‐integrated relining layer on the autologous site
References
-
Mina ElHadidi,Mohamed Mounir,Rofaida A Abaas et al., The International journal of oral & maxillofacial implants. Volume: 0, Issue: 0, 2026
Computer-guided Versus Conventional Modified Cortical Shell Technique for the Rehabilitation of Posterior Mandibular Deficiency: Randomized Controlled Trial.
The cortical shell technique lacks anatomical guidance for harvesting and grafting. This study compares the horizontal bone ga… -
Peer W Kämmerer,Jochen Tunkel,Werner Götz et al., International journal of implant dentistry. Volume: 8, Issue: 1, 2022 The allogeneic shell technique for alveolar ridge augmentation: a multicenter case series and experiences of more than 300 cases.
Allogeneic cortical bone plates (CP) might be used for alveolar ridge augmentation as an alternative to autogenous grafts (AG)… -
Jochen Tunkel,Luca de Stavola,Anita Kloss-Brandstätter et al., Clinical case reports. Volume: 9, Issue: 2, 2021 Alveolar ridge augmentation using the shell technique with allogeneic and autogenous bone plates in a split-mouth design-A retrospective case report from five patients.
Atrophic alveolar ridges of five patients were augmented with allografts and autografts on opposite sites, followed by dental implantation. Both au… -
Romain Doliveux,Simon Doliveux et al., The International journal of oral & maxillofacial implants. Volume: 39, Issue: 2, 2024 Guided and Prosthetically Driven Bone Augmentation Using the Shell Technique and Allogeneic Cortical Plate: A Prospective Case Series.
To describe the use of digital technology to surgically guide the shell technique using allogenic cortical plates for a fully … -
Mohamed Ibrahim Sakr,Mahmoud Hanafy,Amr Gibaly,Mohamed Mounir et al., Clinical implant dentistry and related research. Volume: , Issue: , 2024 Digital workflow for graft harvest and positioning in deficient anterior mandibles versus conventional technique: Randomized controlled trial.
The cortical shell technique is frequently associated with technical drawbacks, such as the lack of anatomical guidance dur… -
Zoran Kovac,Tomislav Cabov,Marko Blaskovic,Luka Morelato et al., Medicina (Kaunas, Lithuania). Volume: 59, Issue: 3, 2023
Regeneration of Horizontal Bone Defect in Edentulous Maxilla Using the Allogenic Bone-Plate Shell Technique and a Composite Bone Graft-A Case Report.
An insufficient volume of the alveolar bone may prevent implants from being placed in the prosthetically optimal position. Complex restoration of b… -
Robert Würdinger,Phil Donkiewicz et al., Journal of esthetic and restorative dentistry : official publication of the American Academy of Esthetic Dentistry … [et al.]. Volume: 32, Issue: 8, 2020
Allogeneic cortical struts and bone granules for challenging alveolar reconstructions: An innovative approach toward an established technique.
The shell technique is a well-established procedure for GBR with which extensive osseous defects can be predictably restored… -
M Korsch et al., Australian dental journal. Volume: 66, Issue: 2, 2021
Tooth shell technique: A proof of concept with the use of autogenous dentin block grafts.
Autogenous bone block graft is considered the gold standard for lateral bony defects. Dentin has been identified to be a su… -
Michael Korsch,Marco Peichl et al., International journal of environmental research and public health. Volume: 18, Issue: 6, 2021
Retrospective Study: Lateral Ridge Augmentation Using Autogenous Dentin: Tooth-Shell Technique vs. Bone-Shell Technique.
In the literature, autogenous dentin is considered a possible alternative to bone substitute materials and autologous bone for certain indications… -
Stefania Andrada Iancu,Daniel Referendaru,Ilinca-Antigona Iancu,Anamaria Bechir,Horia Mihail Barbu et al., Journal of medicine and life. Volume: 15, Issue: 4, 2022
Immediate postoperative complications after lateral ridge augmentation - a clinical comparison between bone shell technique and sticky bone.
Nowadays, implant dentistry is strongly interconnected to bone augmentation procedures. Lateral ridge augmentation is often an imperative treatment… -
Khalid Tarek Karkar,Salah A Metwally,Karim M Abdel Mohsen et al., Annals of maxillofacial surgery. Volume: 13, Issue: 1, 2023 Jan-Jun
Anterior Aesthetic Zone Reconstruction with Allogenic Bone Shell and Autogenous Bone Chips - An Evaluative Study.
Horizontal alveolar bone loss hinders dental implant placement. Reconstruction of alveolar deficiency is mandatory to est… -
Horia Mihail Barbu,Stefania Andrada Iancu,Antonio Rapani,Claudio Stacchi et al., Journal of clinical medicine. Volume: 10, Issue: 17, 2021
Guided Bone Regeneration with Concentrated Growth Factor Enriched Bone Graft Matrix (Sticky Bone) vs. Bone-Shell Technique in Horizontal Ridge Augmentation: A Retrospective Study.
The purpose of this study was to compare clinical results of two different horizontal ridge augmentation techniques: guided… -
Mohamed Mounir,Ola Alaa El Morsy,Hatem Amer,Samy Mounir,Amr Gibaly et al., Oral and maxillofacial surgery. Volume: 25, Issue: 2, 2021
Assessment of bone quality using buccal and palatal autogenous cortical shells harvested from two different mandibular donor sites for maxillary alveolar ridge augmentation: a histomorphometric randomized clinical trial.
This study aims to compare the quality of free autogenous bone grafts harvested from two different mandibular donor sites, use…