To improve clinical outcomes in maxillary sinus augmentation (MSA), several strategies have been suggested. Notably, one of the factors that greatly influences the results of MSA is the choice of bone graft material. It has been suggested that combining the bone graft material with autologous platelet concentrates, such as PRF, may enhance healing. But does PRF help in this specific application? This Week in Dental Implants we are highlighting a new study which showed excellent results by combining xenograft with both liquid PRF (i.e. Sticky Bone) and solid PRF (i.e. PRF membranes) utilizing horizontal centrifugation for PRF creation. (Note: If you are looking for a good Horizontal Machine, please be sure to check out our DALI Horizontal Centrifuge).
Brief Introduction to Platelet-Rich Fibrin (PRF)
Platelet-Rich Fibrin (PRF) is a second-generation platelet concentrate that is derived from the patient’s own blood, making it an autologous biomaterial. PRF is prepared by centrifuging a blood sample without the addition of anticoagulants or other biochemical agents, which differentiates it from Platelet-Rich Plasma (PRP). This process results in a fibrin matrix rich in platelets and leukocytes, which release growth factors and cytokines that aid in the healing process. The advantages of PRF include its ease of preparation, lack of biochemical handling, and its ability to enhance soft and hard tissue healing. 1 For further background on PRF, we highly recommend Platelet-rich fibrin: Basics of biological actions and protocol modifications.
Previous Studies on PRF in Sinus Augmentation Have Been Inconclusive
There have been several studies that have tested the use of PRF to improve outcomes in MSA. These studies have further been collected in meta-analyses.
In the study, Effectiveness of Platelet-Rich Fibrin as an Adjunctive Material to Bone Graft in Maxillary Sinus Augmentation: A Meta-Analysis of Randomized Controlled Trails., the meta-analysis included five randomized controlled trials (RCTs) and assessed various clinical, radiographic, and histomorphometric outcomes. The findings indicated that there were no significant differences in the survival rate of implants, new bone formation, contact between newly formed bone and bone substitute, percentage of residual bone graft, and soft-tissue area between the groups that received PRF and those that did not. 2
Another study, The Effect of Autologous Platelet Concentrates on Maxillary Sinus Augmentation: A Meta-Analysis of Randomized Controlled Trials and Systematic Review. also evaluated the impact of autologous platelet concentrates (APC), in maxillary sinus augmentation procedures and concluded that while the use of APCs in sinus augmentation may shorten the time required for bone graft maturation and allow earlier implant placement, the ability of APCs to improve Bone formation, Implant stability or Bone density all lacked statistical significance. 3
Based on these and other studies, it seems that while PRF show spotential benefits in certain aspects of maxillary sinus augmentation, the evidence is not conclusive, and further standardized research is certainly necessary to determine their true efficacy.
New Study Shows Improved New Bone Formation with PRF Assisted Sinus Augmentation
Despite the inconclusive nature of previous studies, a new study, Sinus Floor Elevation With Platelet-Rich Fibrin From Horizontal Centrifugation and Xenograft: Randomized Clinical Trial. , did show superior bone formation when PRF was combined with deproteinized bovine bone material (DBBM) as compared to those treated with DBBM alone after 4 months of healing. This study seems to be unique in that it used horizontal centrifugation for the creation of PRF, and also used both liquid PRF and solid PRF in the PRF-assisted MSA.
In reviewing the study, while we do not believe the horizontal centrifugation necessarily helped the results (we note significant conflicts of interests in the study in that one author Miron holds intellectual property in the production of platelet‐rich fibrin via horizontal centrifugation), and we think all standard centrifugation techniques, including fixed angle centrifuges, are valid approaches, it seems possible that the addition of both liquid PRF and solid PRF did help in MSA. It seems like previous studies mostly only included the use of PRF membranes and did not use sticky bone, i.e. enhancement of the bone graft material with liquid PRF.
As such we tend to agree with the authors that while additional studies are obviously needed, the current results from this study do suggest that combining graft materials with PRF, by using a solid PRF membrane over a collagen membrane, and mixing the graft materials with liquid PRF, seems to promote improved bone formation post-operatively.
Case Photos from Sinus Floor Elevation With Platelet-Rich Fibrin From Horizontal Centrifugation and Xenograft:
Case photos below provided by:
> Reis GGD, Denardi RJ, de Souza SLS, Silva PHF, Furlaneto F, Miron RJ, Mourão CF, Messora MR. Sinus Floor Elevation With Platelet-Rich Fibrin From Horizontal Centrifugation and Xenograft: Randomized Clinical Trial.
Case below shows comparison between the different protocols following: 1. Standard sinus augmentation with demineralized bovine bone graft (DBBM) vs 2. Sinus augmentation with DBBM + liquid PRF, and a collagen membrane covered with a PRF Membrane. PRF was obtained with horizontal centrifugation.





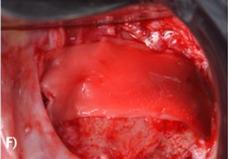
(A) DBBM group—filling of the sinus region with DBBM (Bio‐Oss Large; Geistlich AG, Wolhusen, Switzerland) hydrated in 0.9% saline solution; (B) DBBM group—complete filling of the maxillary sinus; (C) DBBM group—collagen membrane covering the lateral window (BioGide, Geistlich AG, Wolhusen, Switzerland); (D) DBBM + HPRF group—H‐PRF bone block graft after polymerization as a result of the association of solid and liquid DBBM + H‐PRF; (E) DBBM + H‐PRF group—H‐PRF bone block insertion; (F) DBBM + H‐PRF group—H‐PRF membrane covering the collagen membrane (BioGide, Geistlich AG, Wolhusen, Switzerland).
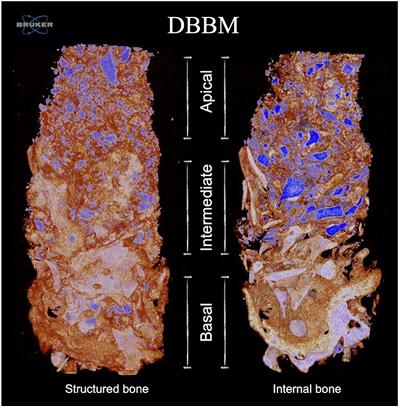
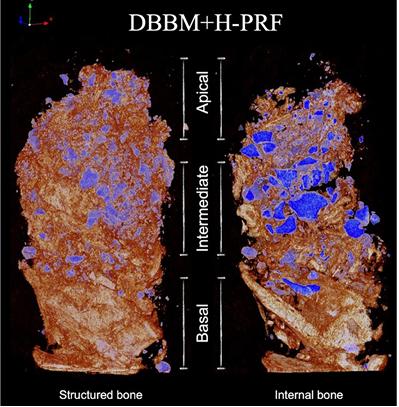
3D Micro‐CT images showing structured bone tissue and internal bone cut of DBBM and DBBM + H‐PRF groups. Remaining bone is depicted in a lighter color in the basal region, NFB is shown in orange throughout the three layers of the biopsies, and the remaining DBBM (xenogeneic bone graft) is depicted in blue in both samples.
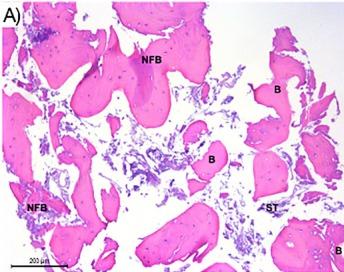
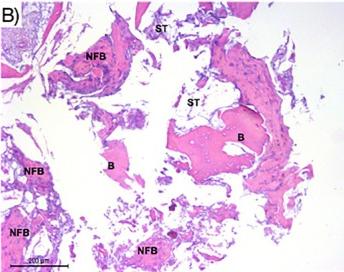
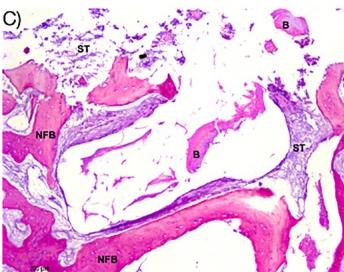
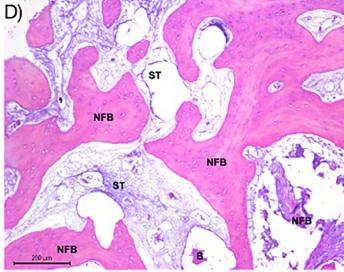
(A) Histological section of the middle‐apical third of the DBBM group demonstrating the presence of biomaterial particles (B) and newly formed bone (NFB). (B) Histological section of DBBM + HPRF group showing widespread presence of osteogenic matrix in NFB, even in more apical areas of the sample, surrounding the biomaterial particles (B). Images (C) and (D) depict the middle third of histological sections of groups DBBM and DBBM + H‐PRF, respectively, demonstrating a noticeable difference in the thickness of NFB between the groups and a difference in the spacing between layers of bone tissue, with the presence of soft tissue (ST) surrounding the biomaterial particles (B).
References
-
Pavlovic V, Ciric M, Jovanovic V, Trandafilovic M, Stojanovic P. Platelet-rich fibrin: Basics of biological actions and protocol modifications. Open Med (Wars). 2021 Mar 22;16(1):446-454.
-
Liu R, Yan M, Chen S, Huang W, Wu D, Chen J. Effectiveness of Platelet-Rich Fibrin as an Adjunctive Material to Bone Graft in Maxillary Sinus Augmentation: A Meta-Analysis of Randomized Controlled Trails. Biomed Res Int. 2019 Mar 17;2019:7267062.
-
Meng Y, Huang X, Wu M, Yang X, Liu Y. The Effect of Autologous Platelet Concentrates on Maxillary Sinus Augmentation: A Meta-Analysis of Randomized Controlled Trials and Systematic Review. Biomed Res Int. 2020 Jun 15;2020:7589072.
-
Reis GGD, Denardi RJ, de Souza SLS, Silva PHF, Furlaneto F, Miron RJ, Mourão CF, Messora MR. Sinus Floor Elevation With Platelet-Rich Fibrin From Horizontal Centrifugation and Xenograft: Randomized Clinical Trial. Clin Implant Dent Relat Res. 2025 Oct;27(5):e70093.