This Week in Dental Implants we are focusing on the role of Hyaluronic acid (HA) in regenerative dentistry.
What is Hyaluronic acid (HA)?
Hyaluronic acid (HA) is a naturally occurring, highly hydrophilic polysaccharide that can be applied in dental and oral‑surgical grafting as a liquid, gel, or cross‑linked formulation. In the studies listed it is used either alone or mixed with bone‑substitutes, collagen matrices, or synthetic membranes.
Is Hyaluronic acid (HA) helpful in regenerative procedures?
Across a range of animal and human studies, as summarized below, HA was shown to:
- reduce dimensional loss of grafted bone,
- increase bone density and new‑bone formation,
- improve soft‑tissue stability and integration,
- accelerate wound healing on donor sites,
- enhance clinical outcomes in peri‑implant disease treatment.
Case Study: Alveolar ridge preservation with hyaluronic acid-enriched allografts
Case below by Frank R Kloss,Thomas Kau,Diana Heimes et al., International journal of implant dentistry. Volume: 10, Issue: 1, 2024 Enhanced alveolar ridge preservation with hyaluronic acid-enriched allografts: a comparative study of granular allografts with and without hyaluronic acid addition..
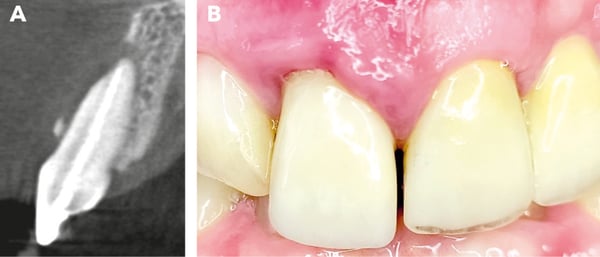
Initial clinical situation. The sectional image of the CBCT, along with the recession on tooth 11, reveals a class III defect according to Kim et al. [3]. The mucosa appears inflamed, and an extensive loss of the buccal alveolar wall is visible

Hyaluronic acid enriched allograft. Figure C shows the allogenic granules mixed with powdered hyaluronic acid. Adding sterile NaCl solution (Figure D) produces a moldable mass known as “sticky bone” (Figure E)
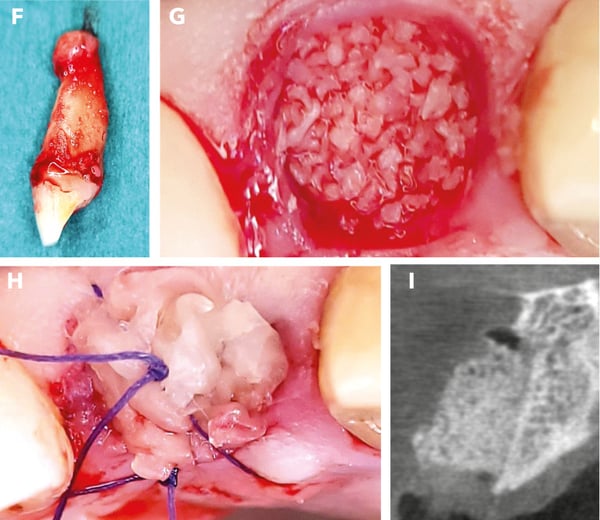
Alveolar ridge preservation. Tooth extraction (Figure F) revealed apical granulation. After mechanical cleaning, the socket was filled with allogenic bone substitute mixed with hyaluronic acid (Figure G). To optimize soft tissue healing, a PRF plug was placed in the socket and secured with a situational suture (Figure H). The postoperative control image (Figure I) shows the vestibular oversizing of the inserted material
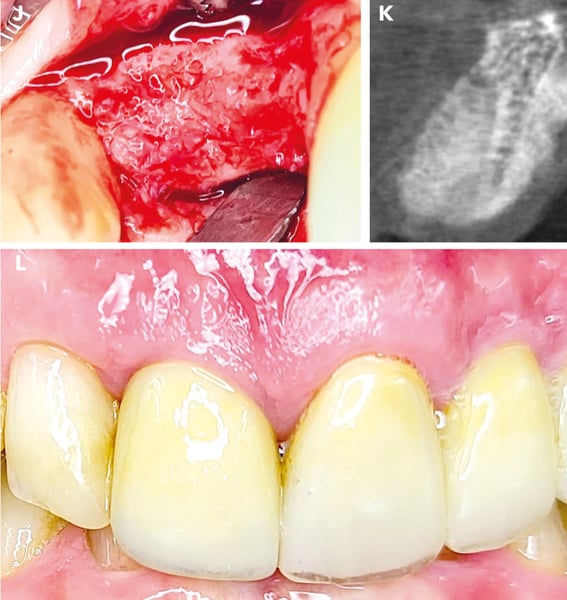
Final situation. After 4 months, when the surgical site was reopened (Figure J), a completely regenerated alveolar ridge was revealed. The alveolus showed complete radiological regeneration (Figure K), allowing for straightforward implant placement. Figure L illustrates the final prosthetic restoration with irritation-free mucosa conditions after one year
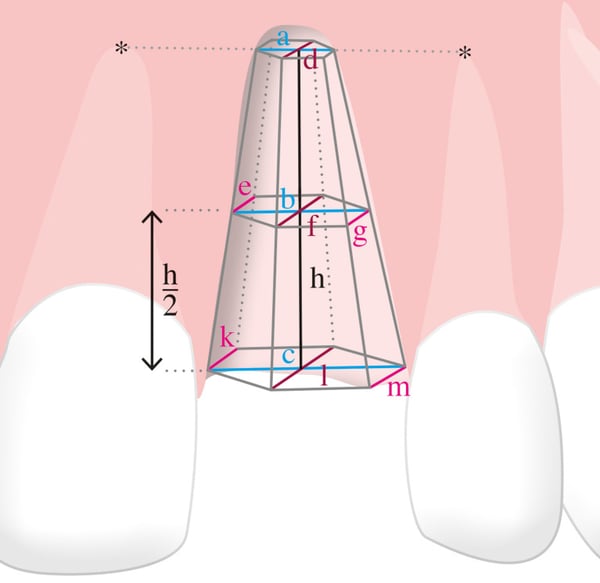
3D-Model for visualizing the mathematical approach of calculating the volume of the defect
In conclusion, our study demonstrates that adding hyaluronic acid to allogeneic bone substitutes in ridge preservation leads to enhanced graft stability, reduced shrinkage rate, and increased bone density. These findings highlight the potential of hyaluronic acid to optimize ridge preservation procedures and promote successful implant integration
Additional Recent Studies
- Clinical and radiographic assessment of cross-linked hyaluronic acid addition in demineralized bovine bone based alveolar ridge preservation: A human randomized split-mouth pilot study.
Bachar Husseini,Anton Friedmann,Ralph Wak,Nabil Ghosn,Georges Khoury,Tala El Ghoul,Chloe Karen Abboud,Ronald Younes et al., Journal of stomatology, oral and maxillofacial surgery. Volume: 124, Issue: 4, 2023
Cross-linked hyaluronic acid (xHyA) appears to limit the post-extractional alveolar bone resorption when mixed with DBBM.
- Boosting angiogenesis experimentally in ovo by biofunctionalizing collagen membranes with platelet-rich fibrin and hyaluronic acid: implications for regenerative oral surgery?
Saskia-Vanessa Schröger,Johanna Becker,Sebahat Kaya et al., International journal of implant dentistry. Volume: , Issue: , 2026
HA also promotes angiogenesis and represents a viable, cost-effective alternative that does not require blood collection. Both PRF and HA biofunctionalization may offer potential benefits for enhancing vascularization in GBR/GTR applications.
- Reconstructive surgical therapy of peri-implant defects with ribose cross-linked collagen matrix and crosslinked hyaluronic acid - a prospective case series. Anton Friedmann,Rico Jung,Hakan Bilhan,Hanan Al Ghawi-Begovic,Frederic Kauffmann,Daniel Diehl et al., Clinical oral investigations. Volume: 28, Issue: 10, 2024
Within the limits of this case series, we conclude that the proposed treatment sequence substantially improved peri-implant defects and offered a simplified but predictive technique. Reconstructive treatment approaches for peri-implantitis are effective but remain non-superior to open flap debridement. Further research on novel biomaterial combinations that may improve reconstructive treatment outcomes are warranted. Ribose-crosslinked collagen matrices biofunctionalized by hyaluronic acid used in this study yield improved clinical and radiographic peri-implant conditions after 12 months.
- Clinical efficacy of hydroxyapatite and tricalcium phosphate modified with hyaluronic acid in the treatment of patients with periimplantitis M M Garunov,L A Grigoriyants,A G Stepanov,S V Apresyan,D V Simonyan et al., Stomatologiia. Volume: 101, Issue: 2, 2022
The results of the study 12 months after the periimplant zone remodeling operation procedure prove the efficacy of HAP and TCF modified with hyaluronic acid for the treatment of patients with periimplantitis.
- Evaluation of the Effect of Hyaluronic Acid Injection on the Reconstruction of Reduced Interdental Papillae in Patients Referred to Shiraz School of Dentistry.
Reihaneh Ebrahimi,Hooman Khorshidi,Rabieh Boroumand,Ali Azadikhah,Pardis Haddadi,Dmd MScD et al., Journal of dentistry (Shiraz, Iran). Volume: 24, Issue: 3, 2023
The effectiveness of using HA gel in reducing the black triangle area was 85.06%. Furthermore, the papilla length increased by 70.256% while contact to papilla distance decreased by 83.026%. At different times, the values of the studied variables in the three levels were significantly different (p< 0.05). Injection of HA with 1.6% concentration at two points of the interdental papilla was effective in interdental papilla reconstruction at the aesthetic zone, especially in long-term, follow-ups (especially 6 months).
- Clinical efficacy of hydroxyapatite and tricalcium phosphate modified with hyaluronic acid in the treatment of patients with periimplantitis M M Garunov,L A Grigoriyants,A G Stepanov,S V Apresyan,D V Simonyan et al., Stomatologiia. Volume: 101, Issue: 2, 2022
The results of the study 12 months after the periimplant zone remodeling operation procedure prove the efficacy of HAP and TCF modified with hyaluronic acid for the treatment of patients with periimplantitis.
- Cyanoacrylate and hyaluronic acid combination on palatal donor site management after de-epithelialized graft harvesting. Hanife Merva Parlak,Murat Haktan Durmaz,Havanur Bayrak,Birtan Tolga Yilmaz,H Gencay Keceli et al., Journal of periodontology. Volume: 94, Issue: 4, 2023
CY application reduces pain and analgesic intake and HA may support the wound healing with increased EL. Using the CY-HA combination provides additional benefits for donor site management.
- Effects of hyaluronic acid and deproteinized bovine bone mineral with 10% collagen for ridge preservation in compromised extraction sockets.
Jun-Beom Lee,Seoyoon Chu,Heithem Ben Amara,Hyun-Young Song,Min-Jung Son,Jungwon Lee,Hae-Young Kim,Ki-Tae Koo,In-Chul Rhyu et al., Journal of periodontology. Volume: 92, Issue: 11, 2021
Ridge preservation with the mixture DBBM-C/HA prevented dimensional shrinkage and improved bone formation in compromised extraction sockets at 1 and 3 months.