This Week in Dental Implants we are highlighting five studies, ranging from Crestal Bone Loss following fixed-implant protheses, GBR with synthetic membranes and graft, the effects of irrigation and other factors on heat during osteotomy, and finally the necessity of re-grafting after a failed sinus lift.
Featured Case: Effect of Fixed Implant-Supported Prosthesis on Crestal Bone Loss
(Case photos below from: Raabe C, Fonseca M, Roccuzzo A, Schimmel M, Salvi GE, Chappuis V, Couso-Queiruga E. Crestal Bone Loss and Peri-Implant Conditions at Tissue-Level Implants: Influence of Prosthesis Type After 25 Years.
The objective of this case study 1 was determine whether the type of implant‑supported fixed dental prosthesis (single crowns [SC], splinted crowns [SP] or bridges [BR]) influences long‑term crestal bone changes (ΔCBL) and the prevalence of peri‑implant mucositis (PM) and peri‑implantitis (PI) around tissue‑level implants after 25 years of function.
Results: After 25 years, the type of prosthesis (single crown, splinted crown or bridge) does not significantly affect crestal bone loss or the prevalence of peri‑implant mucositis or peri‑implantitis around tissue‑level implants. Long‑term bone stability is mainly related to implant location (incisor region), deeper probing depths, and the presence of suppuration, rather than to prosthetic design. 1. Read more about this case.
FIGURE 1.
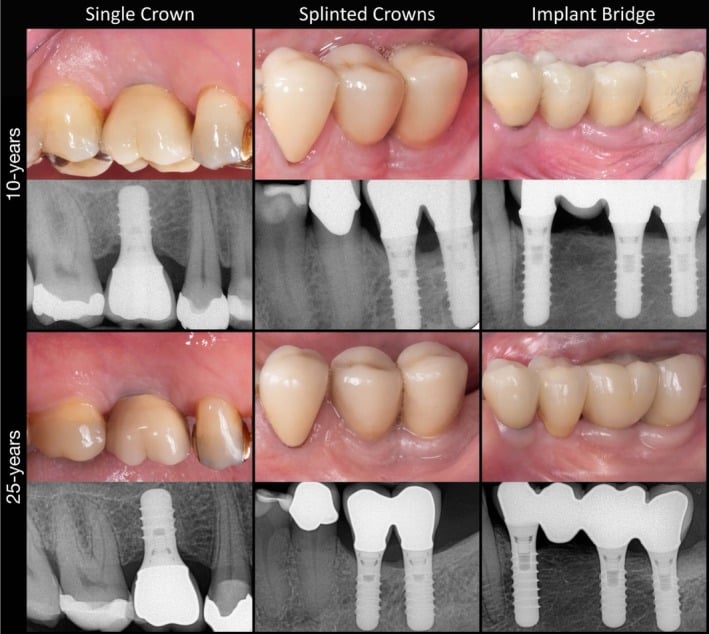
Clinical images and corresponding periapical radiographs of representative cases from each study group at the 10‐year and 25‐year follow‐up. Note that the implant bridge was redone due to chipping.
FIGURE 2.
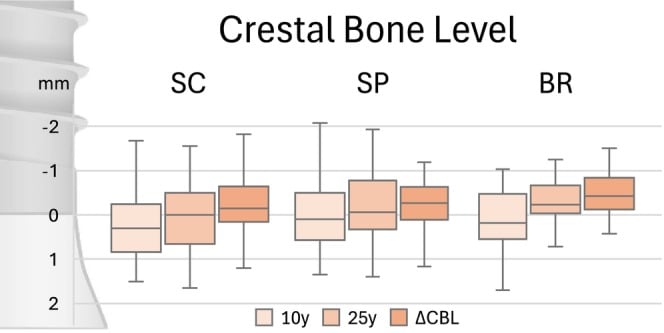
Boxplots of the 10‐ and 25‐year crestal bone levels, as well as the changes depending on the type of implant‐supported prosthesis. BR, Implant bridge; CBL, Crestal bone level; SC, Single implant crowns; SP, Splinted implant crowns.
FIGURE 3.
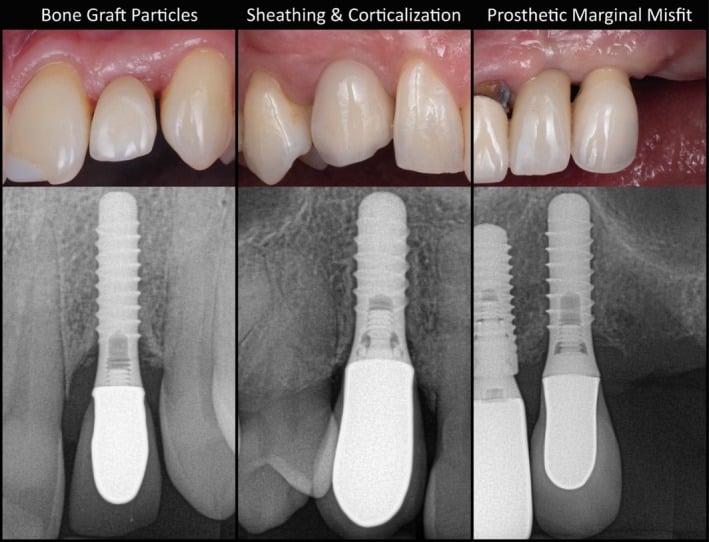
Clinical images and corresponding periapical radiographs of representative cases with adverse radiographic findings
Study: GBR with Synthetic Membranes
This study was done to assess the effectiveness and clinical applicability of guided bone regeneration (GBR) when carbonate apatite granules are combined with poly(lactic acid/caprolactone) (PLCL) membranes in patients with alveolar bone deficiencies. (Note: The synthetic Membranes used in this study are similar to our Cytoflex Resorb membrane). The study concluded:
GBR using carbonate apatite granules and PLCL membranes resulted in significant bone regeneration with low complication rates. This synthetic material combination may offer a reliable approach for GBR. Further studies with larger cohorts and longer follow-up are recommended to validate long-term outcomes and clinical relevance. »Read More 2
Studies on Heat Generation during Osteotomies
Heat generation during implant osteotomy may compromise bone vitality, so these 2 new studies are clinically relevant.
Study: Internal vs External Irrigation
This study was a Systematic review (10 in‑vitro studies) of Internal vs. external vs. combined irrigation. It concluded that: Internal irrigation was consistently more efficient at limiting bone heating than external irrigation, especially in deep osteotomies or when surgical guides were used. Combined irrigation also gave good cooling, but its benefit varied with drill design and experimental setup. » Read More 3
Study: Effect of Osteotomy depth and drill diameter on Heat Generation
This in vitro study evaluated the effects of drill diameter and osteotomy depth on maximum intraosseous temperature (Tmax) and concluded:
Osteotomy depth was the dominant determinant of intraosseous temperature rise, whereas drill diameter had a secondary but clinically relevant effect. Under the tested standardized conditions and continuous irrigation, Tmax remained below the classical 47 °C threshold in all groups. These findings reflect a D1-like cortical model and peak-temperature-only assessment; cumulative thermal dose was not evaluated. » Read More 4
Study: Augmentation After Failed Sinus Floor Elevation?
This study compared the three‑dimensional volumetric shrinkage of endo‑sinus bone grafts around failed versus surviving implants after one‑stage lateral sinus floor elevation (LSFE) and evaluated whether a failed implant can be directly replaced without further augmentation. In concluded that:
Implant failure after LSFE does not necessarily correlate with accelerated resorption of bone graft, supporting the feasibility of direct implant replacement without further grafting. » Read More 5
References
- Raabe C, Fonseca M, Roccuzzo A, Schimmel M, Salvi GE, Chappuis V, Couso-Queiruga E. Crestal Bone Loss and Peri-Implant Conditions at Tissue-Level Implants: Influence of Prosthesis Type After 25 Years. Clin Implant Dent Relat Res. 2026 Jun;28(3):e70158.
- Takahashi A, Ogino Y, Matsuzaki T, Kihara M, Wachi S, Sugi T, Hashiguchi Y, Koyano K, Ayukawa Y. Preliminary clinical evaluation of guided bone regeneration using carbonate apatite granules and poly(lactic acid/caprolactone) membranes: a prospective interventional study. Int J Implant Dent. 2026 May 8.
- Cimini V, Perez A, Shabana H, Di Felice R, Lombardi T. The use of internal irrigation versus external and combined irrigation during dental implant bed preparation, a systematic review. Int J Implant Dent. 2026 May 8.
- Balkanlioğlu AC, Acikan İ. Effect of Osteotomy Depth on Intraosseous Temperature During Implant Drilling: A Standardized CAD/CAM-Guided Thermocouple Study. Int J Oral Maxillofac Implants. 2026 May 6;0(0):1-22.
- Fu M, Zhu D, Song L, Xia Z, Xu W, Jiang Z, Yang G. Long-Term Stability of Bone Graft After Implant Failure in Lateral Sinus Floor Elevation: A Retrospective Paired Study. Clin Implant Dent Relat Res. 2026 Jun;28(3):e70154.